Anda mungkin juga menyukai
- Infection Control for the Dental TeamDari EverandInfection Control for the Dental TeamPenilaian: 5 dari 5 bintang5/5 (1)
- Integrase Inhibitor RaltegravirDokumen15 halamanIntegrase Inhibitor RaltegravirNovi SilitongaBelum ada peringkat
- Viva PathologyDokumen10 halamanViva PathologyKumar KP100% (3)
- Internal Medicine Highlights by Conrad Fischer (2008) PDFDokumen34 halamanInternal Medicine Highlights by Conrad Fischer (2008) PDFLi SacBelum ada peringkat
- Management of Odontogenic Infection of Pulpal and Periodontal OriginDokumen6 halamanManagement of Odontogenic Infection of Pulpal and Periodontal OriginNor Sakinah MBelum ada peringkat
- Jurnal 3 (Biofilm) Fixed PDFDokumen5 halamanJurnal 3 (Biofilm) Fixed PDFNovia SillaBelum ada peringkat
- Oral Biofilms: Molecular Analysis, Challenges, and Future Prospects in Dental DiagnosticsDokumen9 halamanOral Biofilms: Molecular Analysis, Challenges, and Future Prospects in Dental Diagnosticsabcder1234Belum ada peringkat
- Fungal Infections of Oral Cavity: Diagnosis, Management, and Association With COVID-19Dokumen12 halamanFungal Infections of Oral Cavity: Diagnosis, Management, and Association With COVID-19Roxana Guerrero SoteloBelum ada peringkat
- 2 ApikDokumen5 halaman2 ApikAhmad Syauqie Al MuhdarBelum ada peringkat
- Microbiology of Root Canal Infections: Marjut Sakko, Leo Tjäderhane, Riina Rautemaa-RichardsonDokumen6 halamanMicrobiology of Root Canal Infections: Marjut Sakko, Leo Tjäderhane, Riina Rautemaa-Richardsonmarisolporto87Belum ada peringkat
- Antibiotics: Characterization and Antimicrobial Susceptibility of Pathogens Associated With Periodontal AbscessDokumen8 halamanAntibiotics: Characterization and Antimicrobial Susceptibility of Pathogens Associated With Periodontal AbscessAhmed AlhadiBelum ada peringkat
- Endodontic MicrobiologyDokumen11 halamanEndodontic MicrobiologydigdouwBelum ada peringkat
- CALIBR1Dokumen13 halamanCALIBR1Codrin PanainteBelum ada peringkat
- Health Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Dokumen5 halamanHealth Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Kamado NezukoBelum ada peringkat
- Health Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Dokumen5 halamanHealth Notions, Volume 4 Number 2 (February 2020) Issn 2580-4936Kamado NezukoBelum ada peringkat
- Candida-Associated Denture StomatitisDokumen5 halamanCandida-Associated Denture StomatitisAyik DarkerThan BlackBelum ada peringkat
- V37n3a02 en IdDokumen8 halamanV37n3a02 en IdIip RyanBelum ada peringkat
- Bacteriology, Histopathology, Sequelae and Pathogenesis of Oral Mucosal LesionsDokumen24 halamanBacteriology, Histopathology, Sequelae and Pathogenesis of Oral Mucosal LesionsVijetha RaiBelum ada peringkat
- 1 s2.0 S0882401015001527 MainDokumen8 halaman1 s2.0 S0882401015001527 MainAndrei AvîrvareiBelum ada peringkat
- Long-Term Analysis of Resilience of The Oral Microbiome in PDFDokumen13 halamanLong-Term Analysis of Resilience of The Oral Microbiome in PDFGhimpu DanielaBelum ada peringkat
- Seminario Biologia 2Dokumen11 halamanSeminario Biologia 2Daniela Rizo AlvarezBelum ada peringkat
- Shweta PPT ThesisDokumen10 halamanShweta PPT ThesisAKSHAY WAKTEBelum ada peringkat
- J Jdent 2020 103539Dokumen31 halamanJ Jdent 2020 103539Jade SanchezBelum ada peringkat
- Parasite 21 30 PDFDokumen9 halamanParasite 21 30 PDFAziz AkBelum ada peringkat
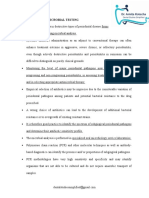
- Microbial Testing Decision MakingDokumen5 halamanMicrobial Testing Decision Makingdr payal bataviaBelum ada peringkat
- Chairside Diagnosis For Plaque AssociatedDokumen7 halamanChairside Diagnosis For Plaque AssociatedMohammed NabeelBelum ada peringkat
- Identificação de Fusobacterium Nucleatum em Infecções Endodônticas Primárias e Secundárias e Sua Associação Com Características Clínicas Usando Dois Métodos DiferentesDokumen10 halamanIdentificação de Fusobacterium Nucleatum em Infecções Endodônticas Primárias e Secundárias e Sua Associação Com Características Clínicas Usando Dois Métodos DiferentesOlimpio Barbosa De Oliveira NetoBelum ada peringkat
- Aerobic and Anaerobic Bacteria in Subgingival and Supragingival Plaques of Adult Patients With Periodontal DiseaseDokumen5 halamanAerobic and Anaerobic Bacteria in Subgingival and Supragingival Plaques of Adult Patients With Periodontal DiseaseRamanda CahyaBelum ada peringkat
- Dentistry 10 00184 1Dokumen12 halamanDentistry 10 00184 1Stefani WijayaBelum ada peringkat
- Diagnostics of Oral Mucosae: Histology and Microbiology - Clinical RelevanceDokumen14 halamanDiagnostics of Oral Mucosae: Histology and Microbiology - Clinical RelevanceGeorgi GugicevBelum ada peringkat
- In Vitro Beneficial Effects of Streptococcus Dentisani As PotentialDokumen10 halamanIn Vitro Beneficial Effects of Streptococcus Dentisani As PotentialValentina Villanueva nietoBelum ada peringkat
- Jcad 13 6 48Dokumen6 halamanJcad 13 6 48neetika guptaBelum ada peringkat
- Resolviendo La Etiologia de La Caries Dental PDFDokumen7 halamanResolviendo La Etiologia de La Caries Dental PDFYesenia Jopia OrellanaBelum ada peringkat
- Mini Review - Mikrobiologi - Real Akbar - 015Dokumen4 halamanMini Review - Mikrobiologi - Real Akbar - 015Real Akbar Aucky SanjayaBelum ada peringkat
- MicrobiologíaDokumen13 halamanMicrobiologíaAlexander TamayoBelum ada peringkat
- Litrev Draft 2 Pages VersionDokumen13 halamanLitrev Draft 2 Pages Versionapi-710900838Belum ada peringkat
- Control of Oral Biofilms: T F. F & T BDokumen7 halamanControl of Oral Biofilms: T F. F & T BGina BBelum ada peringkat
- Symmetry 14 00307Dokumen14 halamanSymmetry 14 00307Phúc BùiBelum ada peringkat
- Dental Research Journal: Microflora and Periodontal DiseaseDokumen5 halamanDental Research Journal: Microflora and Periodontal DiseaseNadya PurwantyBelum ada peringkat
- 2 PBDokumen7 halaman2 PBHenry MandalasBelum ada peringkat
- Pathophysiology of Sinusitis of Odontogenic OriginDokumen7 halamanPathophysiology of Sinusitis of Odontogenic OriginErin NettaBelum ada peringkat
- Articless41368 022 00163 7 PDFDokumen11 halamanArticless41368 022 00163 7 PDFVanessa SmithBelum ada peringkat
- 10.2478 - Cipms 2020 0019Dokumen4 halaman10.2478 - Cipms 2020 0019khamilatusyBelum ada peringkat
- Lactobacillus Salivarius NK02 A Potent Probiotic For ClinicalDokumen11 halamanLactobacillus Salivarius NK02 A Potent Probiotic For ClinicalHossein ShahbaniBelum ada peringkat
- Jurnal Otitis MediaDokumen8 halamanJurnal Otitis MediaAsep Ardi100% (1)
- 4-Australian Dental Journal - 2008 - Figdor - A Big Role For The Very Small Understanding The Endodontic Microbial FloraDokumen14 halaman4-Australian Dental Journal - 2008 - Figdor - A Big Role For The Very Small Understanding The Endodontic Microbial Florakyrillos killineyBelum ada peringkat
- Microbiologi of Chronic Suppurative Otitis MediaDokumen3 halamanMicrobiologi of Chronic Suppurative Otitis MediaDwi Ayu NilamsariBelum ada peringkat
- Influence of Periodontal Treatment On Subgingival and Salivary MicrobiotasDokumen9 halamanInfluence of Periodontal Treatment On Subgingival and Salivary MicrobiotasRabiatul AdawiyahBelum ada peringkat
- 2000 Controlled and Targeted Drug Delivery Strategies Towards Intraperiodontal Pocket DiseasesDokumen22 halaman2000 Controlled and Targeted Drug Delivery Strategies Towards Intraperiodontal Pocket DiseasesK KBelum ada peringkat
- Review Article Candida Species Revealed by High-Throughput TechnologiesDokumen6 halamanReview Article Candida Species Revealed by High-Throughput TechnologiesNovia HartantiBelum ada peringkat
- Endo. MicrobiologyDokumen7 halamanEndo. MicrobiologyzaheerbdsBelum ada peringkat
- Periodontal Disease Research PaperDokumen14 halamanPeriodontal Disease Research Paperapi-397871513Belum ada peringkat
- Caries Vaccine: Guided By: Presented byDokumen5 halamanCaries Vaccine: Guided By: Presented byharishgnrBelum ada peringkat
- Ebook - Antibiotics in Dental Practice How Justified Are WeDokumen7 halamanEbook - Antibiotics in Dental Practice How Justified Are WeNguyễn Quang HuyBelum ada peringkat
- Research Article The Periodontal Abscess: Clinical and Microbiological CharacteristicsDokumen8 halamanResearch Article The Periodontal Abscess: Clinical and Microbiological CharacteristicsdwiariarthanaBelum ada peringkat
- Cariogram Outcome After 90 Days of Oral Treatment With Streptococcus Salivarius M18 in Children at High Risk For Dental Caries Results of ADokumen8 halamanCariogram Outcome After 90 Days of Oral Treatment With Streptococcus Salivarius M18 in Children at High Risk For Dental Caries Results of AShameena KnBelum ada peringkat
- Public Health 309Dokumen5 halamanPublic Health 309Blue TechBelum ada peringkat
- 2428 FullDokumen4 halaman2428 FullEdith TrejoBelum ada peringkat
- Dental Plaque and Carries Formation Week 8.Dokumen12 halamanDental Plaque and Carries Formation Week 8.sima mhammedBelum ada peringkat
- The Oral Microbiome and Human Health: Yoshihisa Yamashita and Toru TakeshitaDokumen6 halamanThe Oral Microbiome and Human Health: Yoshihisa Yamashita and Toru TakeshitaLedy OrduñaBelum ada peringkat
- Oral Candidiasis - ReviewDokumen9 halamanOral Candidiasis - ReviewAdhelia Galuh PrmtsrBelum ada peringkat
- Management and Treatment of Fungal Infection in The Oral CavityDokumen4 halamanManagement and Treatment of Fungal Infection in The Oral CavityKIU PUBLICATION AND EXTENSIONBelum ada peringkat
- Antibiotic Prophylaxis in Pediatric Odontology. An UpdateDokumen6 halamanAntibiotic Prophylaxis in Pediatric Odontology. An UpdateJavier Farias VeraBelum ada peringkat
- English Medical TranslationDokumen11 halamanEnglish Medical Translationlixiaoxiu100% (1)
- Microbiology UW New by FinalstepsDokumen41 halamanMicrobiology UW New by Finalstepsxinfox11Belum ada peringkat
- Community Diagnosis Report Melamchi 2070Dokumen138 halamanCommunity Diagnosis Report Melamchi 2070Shakun6594% (17)
- 2115 Kshudrakusta-VicharchikaDokumen3 halaman2115 Kshudrakusta-VicharchikaSamhitha Ayurvedic ChennaiBelum ada peringkat
- Clinical Scenarios in ICUDokumen107 halamanClinical Scenarios in ICUmatenten100% (4)
- CLAIMS DetailsDokumen8 halamanCLAIMS DetailsZack TanBelum ada peringkat
- CVDokumen4 halamanCVPratistha SatyanegaraBelum ada peringkat
- Health & Hygiene (TSC B&C)Dokumen14 halamanHealth & Hygiene (TSC B&C)egy197183% (24)
- Street SheetDokumen1 halamanStreet SheetKristin McNultyBelum ada peringkat
- Reviewing Harm Reduction For People Who Inject Drugs in Asia - The Necessity For GrowthDokumen5 halamanReviewing Harm Reduction For People Who Inject Drugs in Asia - The Necessity For GrowthAura NirwanaBelum ada peringkat
- Stakeholder AnalysisDokumen10 halamanStakeholder AnalysisashkuchiyaBelum ada peringkat
- Aids CongressDokumen2 halamanAids CongressTin Causaren-GertosBelum ada peringkat
- HUMAN HERPES VIRUS Types 6Dokumen1 halamanHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- Dr. Sadeli Masria, DR., SPMK., Ms. DMMDokumen64 halamanDr. Sadeli Masria, DR., SPMK., Ms. DMMPraluki HerliawanBelum ada peringkat
- ESMO GuidelinesDokumen845 halamanESMO GuidelinesMohamed OsamaBelum ada peringkat
- HIV in Mothers and ChildrenDokumen42 halamanHIV in Mothers and ChildrenDayita ApritutiBelum ada peringkat
- Revolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightDokumen12 halamanRevolutionizing HIV Prevention in Africa Landmark Innovations That Transformed The FightKIU PUBLICATION AND EXTENSIONBelum ada peringkat
- Young Talk, October 2008Dokumen4 halamanYoung Talk, October 2008Straight Talk Foundation100% (6)
- WHO Proforma 5th EditionDokumen41 halamanWHO Proforma 5th EditionMohammed ArshadBelum ada peringkat
- Biology Project Reports On HIV ADokumen5 halamanBiology Project Reports On HIV AManish PatidarBelum ada peringkat
- CHC ChecklistDokumen63 halamanCHC Checklistvibha_bansalBelum ada peringkat
- Peace Corps Namibia Welcome Book - July 2008Dokumen97 halamanPeace Corps Namibia Welcome Book - July 2008Accessible Journal Media: Peace Corps DocumentsBelum ada peringkat
- Steps To Use Routine Information To Improve HIV/AIDS ProgramsDokumen118 halamanSteps To Use Routine Information To Improve HIV/AIDS ProgramsFuturesGroup1Belum ada peringkat
- Motion For Summary Judgment For The Defendant: Fear of Contracting Needlestick CaseDokumen21 halamanMotion For Summary Judgment For The Defendant: Fear of Contracting Needlestick CaseSusan von StruenseeBelum ada peringkat
- Osces For Medical Students, Volume 2 Second EditionDokumen41 halamanOsces For Medical Students, Volume 2 Second EditionNaeem Khan100% (3)
- Millinium Development GoalsDokumen199 halamanMillinium Development GoalsRaghuBelum ada peringkat
- Hiv/Aids: Mwangi KJ (MSC Human Anat)Dokumen47 halamanHiv/Aids: Mwangi KJ (MSC Human Anat)Diana Moraah MoturiBelum ada peringkat