Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- CHAPTER 3 Social Responsibility and EthicsDokumen54 halamanCHAPTER 3 Social Responsibility and EthicsSantiya Subramaniam100% (4)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Perkins 20 Kva (404D-22G)Dokumen2 halamanPerkins 20 Kva (404D-22G)RavaelBelum ada peringkat
- Dr. Dr. Andi Makbul AmanDokumen45 halamanDr. Dr. Andi Makbul AmanSupari CandiBelum ada peringkat
- Chronic Suppurative Otitis MediaDokumen7 halamanChronic Suppurative Otitis MediaSupari CandiBelum ada peringkat
- 9-Medical Expulsive TherapyDokumen4 halaman9-Medical Expulsive TherapySupari CandiBelum ada peringkat
- Be The OneDokumen33 halamanBe The OneSupari CandiBelum ada peringkat
- Office Storage GuideDokumen7 halamanOffice Storage Guidebob bobBelum ada peringkat
- NOP PortalDokumen87 halamanNOP PortalCarlos RicoBelum ada peringkat
- Analysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodDokumen5 halamanAnalysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodleksremeshBelum ada peringkat
- Social Media Marketing Advice To Get You StartedmhogmDokumen2 halamanSocial Media Marketing Advice To Get You StartedmhogmSanchezCowan8Belum ada peringkat
- Delta AFC1212D-SP19Dokumen9 halamanDelta AFC1212D-SP19Brent SmithBelum ada peringkat
- Tivoli Performance ViewerDokumen4 halamanTivoli Performance ViewernaveedshakurBelum ada peringkat
- Wiley Chapter 11 Depreciation Impairments and DepletionDokumen43 halamanWiley Chapter 11 Depreciation Impairments and Depletion靳雪娇Belum ada peringkat
- 4 Bar LinkDokumen4 halaman4 Bar LinkConstance Lynn'da GBelum ada peringkat
- Sky ChemicalsDokumen1 halamanSky ChemicalsfishBelum ada peringkat
- BluetoothDokumen28 halamanBluetoothMilind GoratelaBelum ada peringkat
- POST TEST 3 and POST 4, in ModuleDokumen12 halamanPOST TEST 3 and POST 4, in ModuleReggie Alis100% (1)
- ACIS - Auditing Computer Information SystemDokumen10 halamanACIS - Auditing Computer Information SystemErwin Labayog MedinaBelum ada peringkat
- 2016 066 RC - LuelcoDokumen11 halaman2016 066 RC - LuelcoJoshua GatumbatoBelum ada peringkat
- Form16 2018 2019Dokumen10 halamanForm16 2018 2019LogeshwaranBelum ada peringkat
- Blade Torrent 110 FPV BNF Basic Sales TrainingDokumen4 halamanBlade Torrent 110 FPV BNF Basic Sales TrainingMarcio PisiBelum ada peringkat
- D - MMDA vs. Concerned Residents of Manila BayDokumen13 halamanD - MMDA vs. Concerned Residents of Manila BayMia VinuyaBelum ada peringkat
- Edita's Opertionalization StrategyDokumen13 halamanEdita's Opertionalization StrategyMaryBelum ada peringkat
- Polytropic Process1Dokumen4 halamanPolytropic Process1Manash SinghaBelum ada peringkat
- TSB 120Dokumen7 halamanTSB 120patelpiyushbBelum ada peringkat
- TAB Procedures From An Engineering FirmDokumen18 halamanTAB Procedures From An Engineering Firmtestuser180Belum ada peringkat
- CI Principles of EconomicsDokumen833 halamanCI Principles of EconomicsJamieBelum ada peringkat
- Oracle FND User APIsDokumen4 halamanOracle FND User APIsBick KyyBelum ada peringkat
- Escario Vs NLRCDokumen10 halamanEscario Vs NLRCnat_wmsu2010Belum ada peringkat
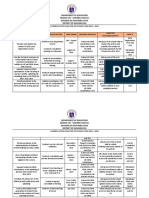
- Action Plan Lis 2021-2022Dokumen3 halamanAction Plan Lis 2021-2022Vervie BingalogBelum ada peringkat
- BSCSE at UIUDokumen110 halamanBSCSE at UIUshamir mahmudBelum ada peringkat
- IEC Blank ProformaDokumen10 halamanIEC Blank ProformaVanshika JainBelum ada peringkat
- ST JohnDokumen20 halamanST JohnNa PeaceBelum ada peringkat
- Electrical ConnectorsDokumen5 halamanElectrical ConnectorsRodrigo SantibañezBelum ada peringkat