Anda mungkin juga menyukai
- The Rate and Indication of Caesarean Section in ADokumen7 halamanThe Rate and Indication of Caesarean Section in AdhananjayBelum ada peringkat
- Jurnal FetoDokumen4 halamanJurnal FetoAl NaifBelum ada peringkat
- JurnalDokumen9 halamanJurnaleeeeeeBelum ada peringkat
- Mitric 2018Dokumen3 halamanMitric 2018Lely WidiawatiBelum ada peringkat
- Obstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalDokumen4 halamanObstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalMohan Kumar DBelum ada peringkat
- Maternal and Fetal Outcome in Oligohydramnios: A Study of 100 CasesDokumen4 halamanMaternal and Fetal Outcome in Oligohydramnios: A Study of 100 Casesria andiniBelum ada peringkat
- Cervical Cerclage and It's Significance in Preventing Second Trimester Abortions Because of Cervical IncompetenceDokumen7 halamanCervical Cerclage and It's Significance in Preventing Second Trimester Abortions Because of Cervical IncompetenceInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Implications of Placenta Previa On Pregnancy Outcome: A Prospective StudyDokumen5 halamanImplications of Placenta Previa On Pregnancy Outcome: A Prospective StudyAisyah Prima PutriBelum ada peringkat
- Guide to Breech Presentation DeliveryDokumen13 halamanGuide to Breech Presentation DeliveryRahmawati Dianing PangestuBelum ada peringkat
- Outcome of Breech Delivery at Term.: Rapid Responses Email AlertingDokumen3 halamanOutcome of Breech Delivery at Term.: Rapid Responses Email AlertingChadik VillanuevaBelum ada peringkat
- Management of Breech PresentationDokumen13 halamanManagement of Breech Presentationdr.Hansen.SH100% (1)
- Journal Homepage: - : Manuscript HistoryDokumen6 halamanJournal Homepage: - : Manuscript HistoryIJAR JOURNALBelum ada peringkat
- A Study On Risk of Twin PregnancyDokumen12 halamanA Study On Risk of Twin PregnancyINDHUMATHI R SUBBUBelum ada peringkat
- Multifetal Pregnancy: Early Diagnosis and ManagementDokumen33 halamanMultifetal Pregnancy: Early Diagnosis and ManagementjasmniaBelum ada peringkat
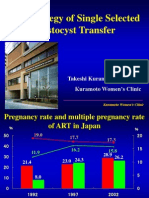
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDokumen43 halamanThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiBelum ada peringkat
- EP Classificationdraft For ReviewDokumen28 halamanEP Classificationdraft For ReviewMaria MogosBelum ada peringkat
- Primary Cesarean Section in MultiparaDokumen3 halamanPrimary Cesarean Section in Multiparapavani pBelum ada peringkat
- Bowel Injury Following Induced Abortion: R.S. Jhobta, A.K. Attri, A. JhobtaDokumen4 halamanBowel Injury Following Induced Abortion: R.S. Jhobta, A.K. Attri, A. JhobtaAle AnzuresBelum ada peringkat
- The clinical characteristics of perineal tears: A study carried out on 14 pregnant women in a tertiaDokumen1 halamanThe clinical characteristics of perineal tears: A study carried out on 14 pregnant women in a tertiaArchemicBelum ada peringkat
- Ectopic PregnancyDokumen27 halamanEctopic PregnancyrowenanuquiBelum ada peringkat
- Multifetal PregnancyDokumen33 halamanMultifetal PregnancyGina Magda RianaBelum ada peringkat
- Ultrasound in Obstet Gyne - 2019 - Litwinska - Outcome of Twin Pregnancy With Two Live Fetuses at 11 13 Weeks GestationDokumen8 halamanUltrasound in Obstet Gyne - 2019 - Litwinska - Outcome of Twin Pregnancy With Two Live Fetuses at 11 13 Weeks GestationIsi Brito AstudilloBelum ada peringkat
- Arabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesDokumen13 halamanArabin Pessary to Prevent Adverse Perinatal Outcomes in Twin Pregnancies With a Short Cervix, PESSARONE. Marion GroussollesqmfddnhdjmBelum ada peringkat
- Evaluation of Pregnancy Outcome Using Usg Scoring SystemDokumen4 halamanEvaluation of Pregnancy Outcome Using Usg Scoring SystemSanjay GoleBelum ada peringkat
- Cerclage Twins EJOGRB 2024Dokumen6 halamanCerclage Twins EJOGRB 2024Willans Eduardo Rosha HumerezBelum ada peringkat
- 15 JMSCRDokumen5 halaman15 JMSCRVani Junior LoverzBelum ada peringkat
- Park 2001Dokumen4 halamanPark 2001witriBelum ada peringkat
- Reech Presentation and Maternal and Perinatal Outcome in A Tertiary Care Teaching Hospital of Central NepalDokumen4 halamanReech Presentation and Maternal and Perinatal Outcome in A Tertiary Care Teaching Hospital of Central NepalSharad GajuryalBelum ada peringkat
- Use of Cervical Length, Measured by Transvaginal Sonography at 22 To 26 Weeks, As A Predictor of Preterm Labour in Twin Pregnancy - 13 Aug 2018Dokumen6 halamanUse of Cervical Length, Measured by Transvaginal Sonography at 22 To 26 Weeks, As A Predictor of Preterm Labour in Twin Pregnancy - 13 Aug 2018Dr B PathakBelum ada peringkat
- Emerging trends in uterine rupture in SingaporeDokumen11 halamanEmerging trends in uterine rupture in SingaporeSulis SipinBelum ada peringkat
- 1 s2.0 S0301211519305822 MainDokumen4 halaman1 s2.0 S0301211519305822 Mainppt.inperBelum ada peringkat
- Cervical pessary reduces preterm birth in twin pregnancies with short cervixDokumen8 halamanCervical pessary reduces preterm birth in twin pregnancies with short cervixjj_cani91Belum ada peringkat
- Materi VBAC Lovamil 202Dokumen30 halamanMateri VBAC Lovamil 202Zoeva VirdiniaBelum ada peringkat
- DynaMed Plus - Premature Rupture of Membranes at Term (Term PROM)Dokumen16 halamanDynaMed Plus - Premature Rupture of Membranes at Term (Term PROM)LudwinBelum ada peringkat
- Preterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudyDokumen9 halamanPreterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudypfannenstielBelum ada peringkat
- Ofir 2003Dokumen5 halamanOfir 2003Jim HawkinsBelum ada peringkat
- A Prospective Study On The Perinatal Outcome in Cases of Previous One Cesarean SectionDokumen4 halamanA Prospective Study On The Perinatal Outcome in Cases of Previous One Cesarean SectionIJAR JOURNALBelum ada peringkat
- Faysal Bas It,+86-89-MinDokumen4 halamanFaysal Bas It,+86-89-MinIT RSMPBelum ada peringkat
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalDokumen4 halamanA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanBelum ada peringkat
- 07 Eo - 16 00005Dokumen6 halaman07 Eo - 16 00005Lenin GutierrezBelum ada peringkat
- The Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterDokumen5 halamanThe Cesarean Section Rate in Cases With Premature Rupture of Membrane (Prom) at 36Th Week of Pregnancy or LaterBob IrsanBelum ada peringkat
- Critical Appraisal Ayu RonoDokumen41 halamanCritical Appraisal Ayu Ronoamarendra WardhanaBelum ada peringkat
- MJCU Volume 86 Issue December Pages 4259-4265Dokumen7 halamanMJCU Volume 86 Issue December Pages 4259-4265SamarBelum ada peringkat
- 1796-Article Text-2702-1-10-20210304 PDFDokumen4 halaman1796-Article Text-2702-1-10-20210304 PDFnoprogamesssBelum ada peringkat
- Vaginal Birth After Cesarean, JurnalDokumen19 halamanVaginal Birth After Cesarean, Jurnaldewi trisnaBelum ada peringkat
- Merced 2019Dokumen14 halamanMerced 2019Vanessa CarinoBelum ada peringkat
- Baru MDokumen3 halamanBaru MRezky Wulandari RoniBelum ada peringkat
- Robsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalDokumen6 halamanRobsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalgehanathBelum ada peringkat
- 2teneurs en Nitrates Dans Les Aquiferes Discontinus Du Socle Du Damagaram Mounio (Est Du Niger)Dokumen7 halaman2teneurs en Nitrates Dans Les Aquiferes Discontinus Du Socle Du Damagaram Mounio (Est Du Niger)IJAR JOURNALBelum ada peringkat
- Uterine Rupture After Previous Caesarean Section: EpidemiologyDokumen12 halamanUterine Rupture After Previous Caesarean Section: EpidemiologymacBelum ada peringkat
- (Zafar Iqba) An Islamic Perspect On GovernanceDokumen28 halaman(Zafar Iqba) An Islamic Perspect On GovernancenazeerahmadBelum ada peringkat
- EJHM - Volume 77 - Issue 3 - Pages 5109-5113Dokumen5 halamanEJHM - Volume 77 - Issue 3 - Pages 5109-5113Andrian drsBelum ada peringkat
- Caesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort StudyDokumen9 halamanCaesarean Birth and Risk of Subsequent Preterm Birth: A Retrospective Cohort Studyluis albenis mendoza guerraBelum ada peringkat
- Perinatal Outcomes After Previable Preterm Premature Rupture of Membranes Before 24 Weeks of GestationDokumen11 halamanPerinatal Outcomes After Previable Preterm Premature Rupture of Membranes Before 24 Weeks of GestationJoseph WilsonBelum ada peringkat
- May 2020 Indications of PCS in Multiparous WomenDokumen4 halamanMay 2020 Indications of PCS in Multiparous WomenTushar BahetiBelum ada peringkat
- Infant Outcome After Complete Uterine RuptureDokumen8 halamanInfant Outcome After Complete Uterine RuptureHeiddy Ch SumampouwBelum ada peringkat
- Obstetrics and Gynecology - 2009Dokumen45 halamanObstetrics and Gynecology - 2009CCGMP100% (1)
- EXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFDokumen8 halamanEXTERNAL CEPHALIC VERSION AND REDUCING THE INCIDENCE OF Breech PDFrolla_hiraBelum ada peringkat
- Jurnal Inggris PDFDokumen4 halamanJurnal Inggris PDFTom PrasBelum ada peringkat
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationDari EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationBelum ada peringkat
- School Communication Flow ChartsDokumen7 halamanSchool Communication Flow ChartsSarah Jane Lagura ReleBelum ada peringkat
- E.Coli Coliforms Chromogenic Medium: CAT Nº: 1340Dokumen2 halamanE.Coli Coliforms Chromogenic Medium: CAT Nº: 1340Juan Manuel Ramos ReyesBelum ada peringkat
- Noise Blinking LED: Circuit Microphone Noise Warning SystemDokumen1 halamanNoise Blinking LED: Circuit Microphone Noise Warning Systemian jheferBelum ada peringkat
- Lecture Notes - Sedimentation TankDokumen45 halamanLecture Notes - Sedimentation TankJomer Levi PortuguezBelum ada peringkat
- IAS Exam Optional Books on Philosophy Subject SectionsDokumen4 halamanIAS Exam Optional Books on Philosophy Subject SectionsDeepak SharmaBelum ada peringkat
- PDF To Sas DatasetsDokumen6 halamanPDF To Sas DatasetsSiri KothaBelum ada peringkat
- Ko vs. Atty. Uy-LampasaDokumen1 halamanKo vs. Atty. Uy-LampasaMaria Janelle RosarioBelum ada peringkat
- D2 Pre-Board Prof. Ed. - Do Not Teach Too Many Subjects.Dokumen11 halamanD2 Pre-Board Prof. Ed. - Do Not Teach Too Many Subjects.Jorge Mrose26Belum ada peringkat
- 1 PPT - Pavement of Bricks and TilesDokumen11 halaman1 PPT - Pavement of Bricks and TilesBHANUSAIJAYASRIBelum ada peringkat
- Wave of WisdomDokumen104 halamanWave of WisdomRasika Kesava100% (1)
- Oral READING BlankDokumen2 halamanOral READING Blanknilda aleraBelum ada peringkat
- Glass Fiber CompositesDokumen21 halamanGlass Fiber CompositesChoice NwikaBelum ada peringkat
- Full Download Test Bank For Macroeconomics 11th Edition Arnold PDF Full ChapterDokumen36 halamanFull Download Test Bank For Macroeconomics 11th Edition Arnold PDF Full Chaptervitalizefoothook.x05r100% (17)
- American Buffalo - DAVID MAMETDokumen100 halamanAmerican Buffalo - DAVID MAMETRodrigo Garcia Sanchez100% (10)
- Drainage Pipe Unit Price AnalysisDokumen9 halamanDrainage Pipe Unit Price Analysis朱叶凡Belum ada peringkat
- StructDokumen2 halamanStructandriessebastianBelum ada peringkat
- Remnan TIIDokumen68 halamanRemnan TIIJOSE MIGUEL SARABIABelum ada peringkat
- Checklist For HR Audit Policy and ProceduresDokumen3 halamanChecklist For HR Audit Policy and ProcedureskrovvidiprasadaraoBelum ada peringkat
- Dalit LiteratureDokumen16 halamanDalit LiteratureVeena R NBelum ada peringkat
- Chrome Settings For CameraDokumen6 halamanChrome Settings For CameraDeep BhanushaliBelum ada peringkat
- IAS 8 Tutorial Question (SS)Dokumen2 halamanIAS 8 Tutorial Question (SS)Given RefilweBelum ada peringkat
- Essay Sustainable Development GoalsDokumen6 halamanEssay Sustainable Development GoalsBima Dwi Nur Aziz100% (1)
- Understanding electromagnetic waves and radioactivityDokumen7 halamanUnderstanding electromagnetic waves and radioactivityJayesh VermaBelum ada peringkat
- History of Filipino Mural (Filipino Americans: A Glorious History, A Golden Legacy)Dokumen9 halamanHistory of Filipino Mural (Filipino Americans: A Glorious History, A Golden Legacy)Eliseo Art Arambulo SilvaBelum ada peringkat
- The Experience of God Being Consciousness BlissDokumen376 halamanThe Experience of God Being Consciousness BlissVivian Hyppolito100% (6)
- Cub Cadet 1650 PDFDokumen46 halamanCub Cadet 1650 PDFkbrckac33% (3)
- Dwnload Full Fundamentals of Human Neuropsychology 7th Edition Kolb Test Bank PDFDokumen12 halamanDwnload Full Fundamentals of Human Neuropsychology 7th Edition Kolb Test Bank PDFprindivillemaloriefx100% (12)
- Affect of CRM-SCM Integration in Retail IndustryDokumen8 halamanAffect of CRM-SCM Integration in Retail IndustryRajeev ChinnappaBelum ada peringkat
- International Waiver Attestation FormDokumen1 halamanInternational Waiver Attestation FormJiabao ZhengBelum ada peringkat
- GVP College of Engineering (A) 2015Dokumen3 halamanGVP College of Engineering (A) 2015Abhishek SunilBelum ada peringkat