Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Dr. Berg's Favorite HEALTHY JUNK FOODS & Other AlternativesDokumen23 halamanDr. Berg's Favorite HEALTHY JUNK FOODS & Other Alternativesprashant_padte100% (8)
- 7) Fusion Accounting Hub For Insurance Premium - External SourceDokumen18 halaman7) Fusion Accounting Hub For Insurance Premium - External Sourcekeerthi_fcmaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- SBI - Certificate To Be Submitted by Pensioner - ChandigarhDokumen1 halamanSBI - Certificate To Be Submitted by Pensioner - ChandigarhMsinghBelum ada peringkat
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Dokumen26 halamanS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- ASTM IndexDokumen34 halamanASTM IndexJimmy Chan67% (3)
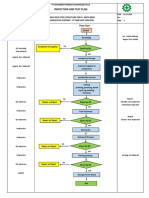
- Inspection and Test Plan: Flow Chart Start IncomingDokumen1 halamanInspection and Test Plan: Flow Chart Start IncomingSinden AyuBelum ada peringkat
- Accredited Meat Processing Plant (MPP) PDFDokumen14 halamanAccredited Meat Processing Plant (MPP) PDFClayton PanghulanBelum ada peringkat
- Rice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian FarmersDokumen2 halamanRice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian Farmersapi-420356823Belum ada peringkat
- Ethnobotany Manual 14th September 2016Dokumen54 halamanEthnobotany Manual 14th September 2016Rahul0% (1)
- Abnegation Faction:: Clothing Is Gray and Simple. The OnlyDokumen7 halamanAbnegation Faction:: Clothing Is Gray and Simple. The OnlylethaagathaBelum ada peringkat
- CASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRDokumen17 halamanCASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRHarry NuryantoBelum ada peringkat
- SAP Technical Consultant resumeDokumen11 halamanSAP Technical Consultant resumeKallol BhowmickBelum ada peringkat
- Sunflower Herbicide ChartDokumen2 halamanSunflower Herbicide ChartpapucicaBelum ada peringkat
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Dokumen15 halamanRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboBelum ada peringkat
- EPF, EPS, Gratuity, Superannuation & Group Life Insurance Nomination FAQsDokumen4 halamanEPF, EPS, Gratuity, Superannuation & Group Life Insurance Nomination FAQsHemanth DhananjayBelum ada peringkat
- Batson Et All - 2007 - Anger and Unfairness - Is It Moral Outrage?Dokumen15 halamanBatson Et All - 2007 - Anger and Unfairness - Is It Moral Outrage?Julia GonzalezBelum ada peringkat
- Volume 1Dokumen168 halamanVolume 1lalitendu jenaBelum ada peringkat
- Soil properties problemsDokumen2 halamanSoil properties problemsAldrin LampareroBelum ada peringkat
- AnxietyDokumen5 halamanAnxietydrmadankumarbnysBelum ada peringkat
- Lab 9-Measurement of Filtrate Loss and Mud Cake Thickness of Drilling Mud Sample Using Dead Weight Hydraulic Filter Press Considering API Standard.Dokumen17 halamanLab 9-Measurement of Filtrate Loss and Mud Cake Thickness of Drilling Mud Sample Using Dead Weight Hydraulic Filter Press Considering API Standard.Sunny BbaBelum ada peringkat
- 01 01Dokumen232 halaman01 01Muhammad Al-MshariBelum ada peringkat
- 12 2022 Salary Slip SintexDokumen1 halaman12 2022 Salary Slip SintexpathyashisBelum ada peringkat
- 9 Oet Reading Summary 2.0-195-213Dokumen19 halaman9 Oet Reading Summary 2.0-195-213Vijayalakshmi Narayanaswami0% (1)
- Mola SubseaDokumen10 halamanMola Subseashahbaz akramBelum ada peringkat
- Catalogo Unidad Enfriadora Trane R-407C PDFDokumen8 halamanCatalogo Unidad Enfriadora Trane R-407C PDFJUAN FRANCISCO AYALABelum ada peringkat
- Product GuideDokumen13 halamanProduct Guidekhalid mostafaBelum ada peringkat
- 2005-05-12Dokumen18 halaman2005-05-12The University Daily KansanBelum ada peringkat
- 3-O FaultDokumen15 halaman3-O FaultJaved Ahmed LaghariBelum ada peringkat
- Afforestation in Arid and Semi Arid RegionsDokumen68 halamanAfforestation in Arid and Semi Arid RegionsMilian Marian SanduBelum ada peringkat
- Solucionario. Advanced Level.Dokumen68 halamanSolucionario. Advanced Level.Christian Delgado RamosBelum ada peringkat