Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Bender Gestalt Visual Motor TestDokumen41 halamanBender Gestalt Visual Motor TestJennifer CaussadeBelum ada peringkat
- Pete Sanders Counselling For DepressionDokumen17 halamanPete Sanders Counselling For DepressionFOCUS Psicología y PsicoterapiaBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Theories of Socialization and PersonalityDokumen36 halamanTheories of Socialization and PersonalityDerick Enage Mabanto100% (3)
- SUICIDE The Call of DarknessDokumen402 halamanSUICIDE The Call of DarknessEmese KovacsBelum ada peringkat
- Crisis & Its InterventionDokumen13 halamanCrisis & Its InterventionAncy Varkey100% (1)
- Daily Nursing AssessmentDokumen2 halamanDaily Nursing Assessmentkiku_laiBelum ada peringkat
- OutputDokumen2 halamanOutputDiaz FarrasizdiharBelum ada peringkat
- Adhi GunawanDokumen5 halamanAdhi GunawanDoyoxBelum ada peringkat
- Uji Coba 1 TTestDokumen6 halamanUji Coba 1 TTestDoyoxBelum ada peringkat
- MM PlotDokumen1 halamanMM PlotDoyoxBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaDoyoxBelum ada peringkat
- 11 (Lengkap Definisi - Talak) PDFDokumen37 halaman11 (Lengkap Definisi - Talak) PDFDoyoxBelum ada peringkat
- APJCP Volume 15 Issue 22 Pages 9575-9578Dokumen4 halamanAPJCP Volume 15 Issue 22 Pages 9575-9578DoyoxBelum ada peringkat
- Prostatitis IfmDokumen44 halamanProstatitis IfmDoyoxBelum ada peringkat
- Full Text 01Dokumen102 halamanFull Text 01DoyoxBelum ada peringkat
- Abr 2014 5 3 67 72 PDFDokumen6 halamanAbr 2014 5 3 67 72 PDFelisabethpriskaBelum ada peringkat
- Ijogr 3 (3) 297-299 PDFDokumen3 halamanIjogr 3 (3) 297-299 PDFDoyoxBelum ada peringkat
- Nejmoa1005419-1Dokumen9 halamanNejmoa1005419-1DoyoxBelum ada peringkat
- Mechanoresponsive Musculoskeletal Tissue Differentiation of Adipose Derived Stem CellsDokumen27 halamanMechanoresponsive Musculoskeletal Tissue Differentiation of Adipose Derived Stem CellsDoyoxBelum ada peringkat
- The Effects of The Local Anesthetics Lidocaine And.20Dokumen6 halamanThe Effects of The Local Anesthetics Lidocaine And.20DoyoxBelum ada peringkat
- ACR 2015 RA GuidelineDokumen25 halamanACR 2015 RA GuidelineAya SorayaBelum ada peringkat
- Alpha Amylase PDFDokumen10 halamanAlpha Amylase PDFnadiaBelum ada peringkat
- ACR AAHKS Perioperative Management GuidelineDokumen14 halamanACR AAHKS Perioperative Management GuidelineDoyoxBelum ada peringkat
- Frid Lund 2016Dokumen20 halamanFrid Lund 2016DoyoxBelum ada peringkat
- Jurnal Plasmodium FalciparumDokumen8 halamanJurnal Plasmodium FalciparumDoyoxBelum ada peringkat
- TuberculosisDokumen6 halamanTuberculosisDoyoxBelum ada peringkat
- Nejmoa1005419-1Dokumen9 halamanNejmoa1005419-1DoyoxBelum ada peringkat
- Respiratory Tract Bacterial Infection Etiological Agents and Susceptibility TestingDokumen8 halamanRespiratory Tract Bacterial Infection Etiological Agents and Susceptibility TestingDoyoxBelum ada peringkat
- Chapter 13 Personality PsychologyDokumen46 halamanChapter 13 Personality Psychologyapi-291179388100% (1)
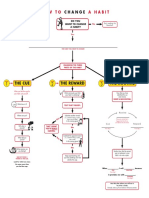
- Flowchart How To Change A Habit PDFDokumen1 halamanFlowchart How To Change A Habit PDFAjit Singh100% (1)
- Disciplines and Ideas in The Social Sciences The Professionals and Practitioners in Counseling Module 3 & 4Dokumen24 halamanDisciplines and Ideas in The Social Sciences The Professionals and Practitioners in Counseling Module 3 & 4Rogel MartizanoBelum ada peringkat
- Somniloquy: Chapter-4 CONSCIOUSNESS Somnabulism/Noctabulism/SleepwalkingDokumen5 halamanSomniloquy: Chapter-4 CONSCIOUSNESS Somnabulism/Noctabulism/SleepwalkingpooriBelum ada peringkat
- How Dancing Helps Your Mental Health: Free-Flowing DanceDokumen4 halamanHow Dancing Helps Your Mental Health: Free-Flowing DanceSasidharan RajendranBelum ada peringkat
- MTQ User Manual 2017 4.00Dokumen66 halamanMTQ User Manual 2017 4.00Ion-Tudor RusuBelum ada peringkat
- Social PerceptionDokumen19 halamanSocial Perceptionamhosny64Belum ada peringkat
- Krause Et Al-2018-Counselling and Psychotherapy ResearchDokumen12 halamanKrause Et Al-2018-Counselling and Psychotherapy ResearchJoaquin OlivaresBelum ada peringkat
- The Shyness and Social Anxiety Workbook For Teens - CBT and ACT Skills To Help You Build Social Confidence by Jennifer Shannon LMFT, Doug Shannon, Christine PadeskyDokumen99 halamanThe Shyness and Social Anxiety Workbook For Teens - CBT and ACT Skills To Help You Build Social Confidence by Jennifer Shannon LMFT, Doug Shannon, Christine PadeskyYulia Afresil100% (1)
- Learned Literature ReviewDokumen8 halamanLearned Literature ReviewMary LearnedBelum ada peringkat
- 6 M's To Keep in Mind When You Next See A Patient With Anorexia NervosaDokumen2 halaman6 M's To Keep in Mind When You Next See A Patient With Anorexia Nervosaaaycee100% (1)
- National Center For Mental Health: (NCMH)Dokumen5 halamanNational Center For Mental Health: (NCMH)Renie SerranoBelum ada peringkat
- Neural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolDokumen2 halamanNeural Retraining Project Highlights: Completion of First Phase Informs Creation of Clinical Trials ProtocolDeepak RanaBelum ada peringkat
- Social Anxiety - Safety BehaviorsDokumen1 halamanSocial Anxiety - Safety BehaviorsMadam KighalBelum ada peringkat
- Behavior ModificationDokumen5 halamanBehavior Modificationapi-315290682Belum ada peringkat
- Introducing Compassion Focused TherapyDokumen10 halamanIntroducing Compassion Focused Therapylwfaxscribd100% (3)
- Mohandas Et Al-2013-British Journal of Dermatology PDFDokumen7 halamanMohandas Et Al-2013-British Journal of Dermatology PDFEdu SajquimBelum ada peringkat
- TRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNDokumen50 halamanTRANSFER, MAINTANENCE, RECOVERY & RELAPSE OF STUTTERING - PDF / KUNNAMPALLIL GEJO JOHNKUNNAMPALLIL GEJO JOHN100% (5)
- Bereavement and GriefDokumen28 halamanBereavement and GriefGeorgiana PrisoschiBelum ada peringkat
- IsbarDokumen2 halamanIsbarKristian Karl Bautista Kiw-isBelum ada peringkat
- Discipline and Ideas in Applied Sciences: Quarter 3 - Module 2Dokumen21 halamanDiscipline and Ideas in Applied Sciences: Quarter 3 - Module 2Lindesol SolivaBelum ada peringkat
- PANSSDokumen2 halamanPANSSShawn MooneyBelum ada peringkat
- Classification of Mental Disorders: A Global Mental Health PerspectiveDokumen4 halamanClassification of Mental Disorders: A Global Mental Health PerspectiveKabeloBelum ada peringkat
- Huntingtons Disease ProjectDokumen9 halamanHuntingtons Disease Projectapi-306544419Belum ada peringkat