Brachial Plexopathies, Classification, Causes and Consequences (Muscle and Nerve, 2004)
Diunggah oleh
Nishki GejmerHak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Brachial Plexopathies, Classification, Causes and Consequences (Muscle and Nerve, 2004)
Diunggah oleh
Nishki GejmerHak Cipta:
Format Tersedia
INVITED REVIEW ABSTRACT: The brachial plexus, which is the most complex structure of
the peripheral nervous system, supplies most of the upper extremity and
shoulder. The high incidence of brachial plexopathies reects its vulnerabil-
ity to trauma and the tendency of disorders involving adjacent structures to
affect it secondarily. The combination of anatomic, pathophysiologic, and
neuromuscular knowledge with detailed clinical and ancillary study evalua-
tions provides diagnostic and prognostic information that is important to
clinical management. Since most brachial plexus disorders do not involve
the entire brachial plexus but, rather, show a regional predilection, a regional
approach to assessment of plexopathies is necessary.
Muscle Nerve 30: 547568, 2004
BRACHIAL PLEXOPATHIES: CLASSIFICATION,
CAUSES, AND CONSEQUENCES
MARK A. FERRANTE, MD
Department of Neurology, Tulane University Medical Center, New Orleans, Louisiana, USA
Accepted 1 June 2004
The brachial plexus, which supplies most of the clinically (e.g., anconeus), recognize minimally af-
upper extremity and shoulder, is the most complex fected muscles that seem normal clinically, prove
structure in the peripheral nervous system (PNS). Its continuity when visible muscle movement is lacking,
vulnerability to trauma reects its large size, super- recognize remote lesions no longer appreciable clin-
cial location, and position between two highly mo- ically, and estimate lesion severity for current and
bile structures (neck and upper extremity).121,144 future comparative studies.
Also, it may be affected secondarily by pulmonary, By integrating requisite anatomic, pathophysio-
vascular, or skeletal disorders involving neighboring logic, and neuromuscular knowledge with detailed
structures. Hence, most physicians encounter pa- clinical assessment and the results of ancillary stud-
tients with brachial plexopathies. In addition to a ies, the examining physician can make an accurate
comprehensive clinical evaluation, optimal assess- diagnosis and prognosis. The lesion must be local-
ment requires the performance of ancillary studies. ized and characterized. This ability requires an un-
Of these, electrodiagnostic examination is by far the derstanding of the relevant anatomy, as well as a
most helpful. Although an extension of the neuro- familiarity with disorders affecting the brachial
logic examination, it has several advantages over the plexus. This review details a regional approach to
latter, including the ability to localize and character- assessment of the brachial plexus and discusses cer-
ize the lesion, evaluate muscles not easily assessed tain plexopathies, especially those with a regional
proclivity. Pertinent aspects of the anatomy, pathol-
ogy, pathophysiology, electrodiagnosis, and injury
Abbreviations: ADM, abductor digiti minimi; AHC, anterior horn cell; APB, classication of these disorders are reviewed.
abductor pollicis brevis; CMAP, compound muscle action potential; CSF,
cerebrospinal uid; CT, computerized tomography; DRG, dorsal root gan-
glion; DUC, dorsal ulnar cutaneous; EDC, extensor digitorum communis; EIP,
extensor indicis proprius; EPB, extensor pollicis brevis; FDI, rst dorsal in- ANATOMY
terosseous; LABC, lateral antebrachial cutaneous; MABC, medial antebra-
chial cutaneous; MR, magnetic resonance; MUAP, motor unit action poten- The brachial plexus is a triangular-shaped structure
tial; NA, neuralgic amyotrophy; NCS, nerve conduction study; NEE, needle
electrode examination; PNS, peripheral nervous system; SNAP, sensory
that extends from the spinal cord to the axilla. Its
nerve action potential; TOS, thoracic outlet syndrome average extraforaminal length is 15.3 cm.117 It is
Key words: brachial plexus, classic postoperative paralysis, electrodiagnos-
tic evaluation, iatrogenic plexopathy, medial brachial fascial compartment,
composed of connective and neural tissue in a 2 to 1
neoplastic plexopathy, neuralgic amyotrophy, obstetric plexopathy, plexopa- ratio,9,117,154 and contains several elements: (1) ve
thy, Pancoast syndrome, postmedian sternotomy, radiation plexopathy, root
avulsion, rucksack, thoracic outlet syndrome, trauma roots (classically, C5 through T1); (2) three trunks
Correspondence to: M. A. Ferrante, 1720-A Medical Park Drive, Suite 210, (upper, middle, and lower); (3) six divisions (three
Biloxi, MS 39532, USA; e-mail: mferrante@bienvilleortho.com
anterior, three posterior); (4) three cords (lateral,
2004 Wiley Periodicals, Inc.
Published online 27 September 2004 in Wiley InterScience (www.interscience.
posterior, and medial); and (5) several terminal
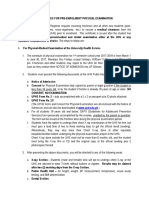
wiley.com). DOI 10.1002/mus.20131 nerves (Fig. 1). The C6, C7, and C8 roots each
Brachial Plexopathies MUSCLE & NERVE November 2004 547
FIGURE 1. The brachial plexus.
provide about 25% of its nerve bers, and the C5 cles. Preganglionic sympathetic bers leave the spi-
and T1 roots provide the remainder.117 The percent- nal cord and exit the anterior primary rami, via white
age of sensory and motor bers composing each root rami communicantes, to reach the sympathetic gan-
varies. The largest percentage of motor bers is glia. The sympathetic ganglia send postganglionic
found in the C5 and C6 roots; C7 and T1 have the bers, via gray rami communicantes, to the C5
least.46,154 The greatest number of sensory bers is through T1 spinal nerves. Although anatomists de-
found in the C7 root, followed, in descending order, ne the anterior primary rami as the roots of the
by C6, C8, T1, and C5.154 The brachial plexus also brachial plexus, much of the surgical literature de-
carries sympathetic bers. nes them as those PNS elements proximal to the
trunks.144 Because of its clinical utility, the latter
Roots. The dorsal and ventral rootlets exit the spi- approach is used in this article.
nal cord and fuse, forming the dorsal and ventral
roots, respectively. The latter enter the interverte- Trunks. The trunks are located in the posterior
bral foramen and fuse in the distal foramen, just cervical triangle, behind the clavicle and sternoclei-
beyond the dorsal root ganglion (DRG), creating a domastoid. Trunk anomalies are infrequent.75 Typi-
spinal nerve. (The latter are also referred to as cally, the C5 and C6 anterior primary rami unite, the
mixed spinal nerves because they contain both sen- C7 anterior primary ramus continues, and the C8
sory and motor nerve bers.) After exiting the fora- and T1 rami coalesce to become the upper, middle,
men, these nerves give off posteriorly directed and lower trunks, respectively (named for their re-
branches, the posterior primary rami, and continue lationship to each other). The upper trunk gives off
as anterior primary rami (Fig. 2). The anterior pri- the suprascapular nerve and the nerve to the subcla-
mary rami emerge from between the anterior and vius muscle. The lower trunk lies adjacent to the
middle scalene muscles. The long thoracic nerve subclavian artery and the apex of the lung.
(serratus anterior) is derived via branches from the
C5C7 anterior primary rami, the C5 ramus contrib- Divisions. Each trunk divides into anterior and pos-
utes to the phrenic (diaphragm) and dorsal scapular terior divisions, all of which are retroclavicular. The
(levator scapulae; rhomboids) nerves, and the anterior and posterior divisions primarily supply
C5C8 rami supply the scalene and longus colli mus- exor and extensor muscles, respectively. Although
548 Brachial Plexopathies MUSCLE & NERVE November 2004
the anterior and posterior divisions of the upper of the upper extremity. Narakas dened that point at
trunk are similar in caliber, the posterior division of 3 cm beyond the cord, but Wilbourn prefers to
the middle trunk is much larger (C7 extensors) than consider the transition site as the point where they
its anterior division,154 whereas the posterior division exit the axilla.95,148
of the lower trunk is much smaller (C8 T1 exten- Classically, the brachial plexus is dened as con-
sors) than its anterior counterpart. When present, sisting of sensory and motor nerve bers derived
less than 5% of posterior cord bers are T1-de- from neurons located in the C5T1 DRG and ante-
rived.52,117 Nerves usually do not arise from the divi- rior horn cells (AHCs), respectively.16,125 However,
sions. vertical variations in its composition are not uncom-
mon. When adjacent roots contribute (e.g., C4, T2),
Cords. The cords are named for their relationship it is expanded. Vertical shifts result when its for-
to the second segment of the axillary artery, to which mation is shifted one level upward or downward.
typically they are bound (Fig. 3). They form at or just When the C4 contribution is large and the T1 con-
beyond the clavicle, below the pectoralis minor, and tribution is small, the brachial plexus is said to be
lie in the proximal region of the axilla, near the pre-xed, and when the C5 contribution is mini-
axillary lymph node chain and major blood vessels to mal and the T2 contribution is large it is post-xed.
the arm.16,20,47,138,148 The lateral cord, formed from Since these one-segment shifts do not affect the
the anterior divisions of the upper and middle plexus arrangement itself, they do not affect lesion
trunks, contains C6 C7 sensory and C5C7 motor localization by either clinical or electrodiagnostic
bers. No C5 sensory bers exist in the lateral cord, examination.
since the C5 dermatome is subserved by the upper
and lower lateral cutaneous nerves, which derive CLASSIFICATION OF BRACHIAL PLEXOPATHIES
from the axillary and radial nerves, respectively;
these nerves exit from the posterior cord. The lateral Brachial plexopathies can be classied in several
cord gives off the lateral pectoral and musculocuta- ways. They are best classied according to the region
neous nerves and terminates as the lateral head of involved, such as supraclavicular (root and trunks),
the median nerve. The posterior cord, formed by retroclavicular (divisions), and infraclavicular (cords
union of the three posterior divisions, contains and terminal nerves) sites. (Isolated retroclavicular
C5C7 sensory and C5C8 motor bers; it does not plexopathies are rare.) Although this approach is
contain C8 sensory bers.27 It gives off the subscap- anatomically simple, it has considerable clinical util-
ular and thoracodorsal nerves before terminating as ity because the incidence, severity, prognosis, and
the axillary and radial nerves. The medial cord, a lesion type vary among these regions.144 In general,
direct continuation of the anterior division of the supraclavicular plexopathies are more common,
lower trunk, contains C8 and T1 sensory and motor more frequently due to closed traction (which can
bers. It gives off the medial pectoral, medial bra- produce lengthy lesions), usually more severe (since
chial cutaneous, medial antebrachial cutaneous greater force is required to produce them), and
(MABC), and ulnar nerves, and terminates as the typically associated with a worse outcome.1,7,66,144
medial head of the median nerve. When the lateral The supraclavicular plexus is further divided into
cord or C7 root sends nerve bers to the ulnar nerve, upper (C5 and C6 roots and upper trunk), middle
C7 radiculopathies can produce abnormalities in (C7 root and middle trunk), and lower (C8 and T1
ulnar-innervated muscles (e.g., exor carpi ul- roots and lower trunk) portions and, again, this is a
naris).20,45,62,117 clinically relevant distinction. Patients with upper
plexopathies tend to recover more completely be-
Terminal Nerves. These elements are located in the cause, in general, these lesions are more commonly
distal axilla and, depending on the author, number due to demyelinating conduction block, located
from three (median, ulnar, and radial) to ve (in- closer to the muscles they innervate, and extrafo-
clusion of musculocutaneous and axillary). Except raminal (i.e., surgically accessible). This classica-
for the median nerve (derived from lateral and me- tion system facilitates communication among physi-
dial cords), these nerves originate from a single cians since it is easier to discuss a patient with an
cord: the ulnar nerve from the medial cord, the upper plexopathy than to commit to one of its ele-
axillary and radial nerves from the posterior cord, ments before diagnostic testing has been performed
and the musculocutaneous nerve from the lateral or when there are examination limitations (e.g.,
cord. It is unclear at which point the terminal nerves pain, mental status changes, or nonneural injuries,
of the brachial plexus become the peripheral nerves such as fractures or dislocations). The infraclavicular
Brachial Plexopathies MUSCLE & NERVE November 2004 549
FIGURE 2. The relationship between the more proximal elements of the brachial plexus and the spinal column.
plexus is not subdivided because lesions affecting it ASSESSMENT OF THE BRACHIAL PLEXUS
do not show signicant regional differences in inci- Clinical Assessment. A detailed clinical evaluation
dence, severity, prognosis, or lesion type. is vital for determining lesion localization (especially
FIGURE 3. The relationship between the brachial plexus and its neighboring arteries.
550 Brachial Plexopathies MUSCLE & NERVE November 2004
its proximal extent) and severity (complete or in- Despite its drawbacks (monoplanar imaging;
complete), both of which have diagnostic and prog- beam-hardening artifacts; poor tissue differentia-
nostic implications that contribute to clinical man- tion), computerized tomography (CT) scanning is
agement. The initial and subsequent symptoms, the useful for identifying bony changes and acute collec-
circumstances surrounding their onset (e.g., back- tions of blood.35 Very thin slice (2-mm) CT-myelog-
pack usage; severe shoulder pain, followed by muscle raphy images the axially oriented preganglionic root
weakness and wasting; postmedian sternotomy; axil- elements when nerve root avulsion is suspected.119
lary or scalene block anesthesia), and the past med- When the meninges are pulled through the neural
ical history are reviewed. In the setting of trauma, foramen, a contrast-lled meningeal diverticulum
arm position at impact suggests the bers most likely may be observed. The width of the dye column in the
affected, as may concomitant injuries (e.g., scapular, cervical gutter is assessed for narrowing (spinal cord
clavicular, or humeral fracture; glenohumeral dislo- edema) and thickening (spinal cord atrophy), and
cation; scapulothoracic dissociation).156 Since most the intraspinal canal is assessed for masses. De-
brachial plexopathies are axon loss in nature, neu- formed dural pouches, poor root sleeve lling, and
rologic examination frequently discloses weakness cord edema or atrophy have strong correlations with
and sensory loss. With supraclavicular lesions, the root avulsion.2,66,119,130 To lessen the chance of
pattern of sensory and motor loss is segmental arachnoiditis, these studies usually are performed
dermatomal and myotomal, respectivelywhereas 4 6 weeks after symptom onset in those patients
infraclavicular plexopathies produce nonsegmental with persistent decits.119 As with other studies,
patterns that resemble those observed with involve- falsely positive (e.g., extraforaminal injuries, menin-
ment of one or more terminal nerves. The presence geal tearing without root damage) and negative
of a Horners syndrome or involvement of the (e.g., after healing and scarring of the dural pouch)
phrenic, dorsal scapular, or long thoracic nerve in- results occur.20,56,63,86,93,107,108,130,156,158 The reliability
dicates a proximal process and portends a worse of CT-myelography is greatest for C8 and T1 avul-
prognosis. Dysautonomic features, such as cutaneous sions.50
trophic changes, sudomotor abnormalities, and va- Its noninvasiveness, lack of radiation, multiplanar
somotor abnormalities, may also be noted. Clinical imaging, lack of degradation by bone, and, espe-
features strongly correlated with root avulsion in- cially, its tissue differentiating ability make magnetic
clude severe pain in an anesthetic limb and Horners resonance (MR) imaging the modality of choice for
syndrome. When traumatic plexopathies are en- more distal brachial plexus imaging. Although it is
countered, spinal accessory nerve, cervical plexus, becoming more widely used for proximal brachial
and phrenic nerve function require assessment. plexus assessment, a recent study comparing it to
CT-myelography found it less sensitive for avulsion
Radiologic Assessment. The radiologic procedures injuries.11 Unfortunately, when multiple slices and
employed reect the circumstances (e.g., urgency, planes are required, acquisition time can be consid-
suspected etiology and lesion site, availability). Plain erable. Magnetic resonance myelography is a newer
lms of the cervical spine, scapula, clavicle, hu- technique that generates myelogram-like images of
merus, shoulder, and chest assess for concomitant the intraspinal canal and intervertebral foramina via
injuries and, with open injuries, for foreign bodies.75 the three-dimensional reconstruction of T2-weighted
Signs of phrenic nerve dysfunction (e.g., elevated images of the cerebrospinal uid (CSF).70,129 Trau-
diaphragm), vascular trauma (e.g., mediastinal wid- matic meningoceles and injuries involving the C5 or
ening), or lung breach (e.g., pneumothorax, hemo- C6 spinal nerves can be visualized. Since it is nonin-
thorax) are sought. Radiologic features associated vasive, contrast-free, relatively quick, and multipla-
with brachial plexus injury include lateral tilt of the nar, this technique could become a useful adjunct
cervical spine and fractures of the transverse process, for assessing proximal brachial plexus elements.150
proximal rst rib, or neighboring bones with root Magnetic resonance neurography can image pe-
avulsion injuries; nonunion or excessive callus for- ripheral nerves using diffusion neurography or T2-
mation with inadequately treated midshaft clavicular based neurography.31 With diffusion neurography,
fractures; humeral fracture or glenohumeral disloca- tissue differentiation reects water diffusion differ-
tion with infraclavicular plexopathies; bone or lung ences rather than T1 or T2 differences. Tissue
abnormalities with neoplastic or radiation damage; brightness is determined by the extent to which
and rudimentary cervical ribs or elongated C7 trans- protons in that tissue are able to spin at exactly the
verse processes with true neurogenic thoracic outlet same rate and in phase with one another. Since the
syndrome (TOS).150 water molecules within a nerve diffuse longitudi-
Brachial Plexopathies MUSCLE & NERVE November 2004 551
nally, application of a perpendicular magnetic eld plexopathies have a regional predilection, lesion lo-
gradient allows these molecules to experience a uni- calization may have diagnostic implications. Thus,
form and unchanging eld strength, thereby causing whenever a plexopathy is suspected, extensive sen-
the nerve to appear increasingly bright in relation to sory NCS are performed. Conversely, since motor
any surrounding tissue. Unfortunately, this tech- NCS are quite insensitive to axon loss and are nor-
nique is very sensitive to patient motion.31 In addi- malized by reinnervation, they are not useful for
tion, since sagittal images are not truly perpendicu- screening purposes. During the rst week, before
lar to the plexus elements, identication and compound muscle action potential (CMAP) ampli-
evaluation of the latter can be difcult.85 With T2- tudes reach their nadir, motor NCS can localize both
based neurography, T2-weighting and both fat and axonal and demyelinating conduction-block lesions;
blood suppression, as well as voxel shortening, per- subsequently, they can only localize the latter, which
mit intraneural fascicles to be imaged. Although
permits differentiation between the two processes.
these techniques can localize neural lesions, they
Another use of motor NCS is for estimating lesion
work best when they are directed to a specic region
severity. Before reinnervation, the relationship be-
by clinical or electrodiagnostic ndings. In the
tween CMAP amplitude and the number of motor
proper setting, MR neurography may be able to
recognize nerve discontinuities and ball neuromas bers is nearly linear. This allows side-to-side CMAP
(e.g., upper trunk disruption), nerve deections amplitude comparisons to estimate the percentage
(e.g., lower trunk angulation caused by a brous of motor bers affected. Due to the large number of
band), and primary nerve tumors (e.g., schwanno- brillation potentials generated per disrupted axon,
mas).31 the NEE is the most sensitive indicator of motor
axon loss. This sensitivity is invaluable for determin-
Vascular Assessment. Brachial plexus damage may ing the proximal extent of a lesion. Also, since it
follow subclavian or axillary vessel damage (e.g., an- studies individual motor unit action potentials
eurysms, pseudoaneurysms, hematomas). Thus, arte- (MUAPs), it can determine continuity and identify
riographic studies often are required, especially early reinnervation when there is no muscle move-
when the plexopathy follows a penetrating injury, ment clinically. Moreover, when discordance be-
coexists with or was caused by a primary vessel injury, tween temporal and spatial MUAP recruitment is
or when examination discloses absence of the radial noted, it can identify the presence of a more proxi-
or carotid pulse or an expanding mass, bruit, or mally located demyelinating conduction-block le-
thrill near the injury site.66,150 Since the distractive sion.
force required to produce neurovascular injury is Since brachial plexus elements are composed of
greater than that to produce isolated neurologic nerve bers derived from different spinal cord seg-
damage, the prognosis for nerve recovery is less fa- ments, lesions involving individual elements have
vorable when it is associated with concomitant vas- different electrodiagnostic features. The muscle
cular involvement66
domain of a brachial plexus element is dened as
the muscles innervated by the motor bers
Electrodiagnostic Assessment of the Brachial Plexus. contained within it. These domains are easily calcu-
Electrodiagnostic assessment of brachial plexopa- lated from standard myotomal charts (Table
thies is invaluable for determining lesion severity 1).27,28,30,61,82,83,102,121,149 The CMAP and SNAP do-
and location, which have important diagnostic and
mains of an element are determined by the sensory
prognostic implications. In general, extensive nerve
and motor bers contained within that element and
conduction study (NCS) and needle electrode exam-
whether they are assessable by NCS.27,30 Thus, the
ination (NEE) evaluations are required, in addition
CMAP domains are a subset of the muscle domains
to contralateral comparison studies. When ap-
proached regionally, however, the requisite number (Table 2).28,30 Since the sensory nerve bers subserv-
of studies is reduced. Sensory NCS, motor NCS, and ing the various sensory NCS do not necessarily arise
NEE are all required because each yields informa- from the same DRG, the pathways through the
tion not discerned by the other two. On NCS, the plexus traversed by these bers varies. For that rea-
sensory nerve action potential (SNAP) amplitudes son, the SNAP domains of the brachial plexus ele-
are the most useful indicators of an axon-loss bra- ments also vary. These pathways and the frequency
chial plexopathy. In addition to differentiating pre- with which brachial plexus elemental lesions affect
and postganglionic lesions, the pattern of SNAP ab- the various SNAPs have been described elsewhere
normalities has localizing value. And, since many (Table 3).27,28,30
552 Brachial Plexopathies MUSCLE & NERVE November 2004
Table 1. Muscle domains of the brachial plexus elements.*
Upper trunk Middle trunk Lower trunk
Supraspinatus Pronator teres Abductor pollicis brevis
Infraspinatus Flexor carpi radialis Flexor pollicis longus
Biceps Triceps Pronator quadratus
Deltoid Anconeus Extensor indicis proprius
Teres minor Extensor carpi radialis Extensor pollicis brevis
Triceps Extensor digitorum communis Extensor carpi ulnaris
Pronator teres First dorsal interosseous
Flexor carpi radialis Abductor digiti minimi
Brachioradialis Adductor pollicis
Extensor carpi radialis Flexor digitorum profundus 4,5
Brachialis Flexor carpi ulnaris
Lateral cord Posterior cord Medial cord
Biceps Latissimus dorsi Abductor pollicis brevis
Brachialis Deltoid Opponens pollicis
Pronator teres Teres minor Flexor pollicis longus
Flexor carpi radialis Triceps First dorsal interosseous
Anconeus Adductor pollicis
Brachioradialis Abductor digiti minimi
Extensor carpi radialis Flexor carpi ulnaris
Extensor digitorum communis Flexor digitorum profundus 4,5
Extensor pollicis brevis
Extensor carpi ulnaris
Extensor indicis proprius
*Only muscles easily assessed by needle electrode examination are listed.
Sensory Fiber Pathways. The lateral antebrachial and DRG (Fig. 4). The sensory bers of the median
cutaneous (LABC) nerve, which exits from the lat- nerve have particularly complicated pathways
eral cord, is the terminal portion of the musculocu- through the brachial plexus. Those innervating the
taneous nerve. Its sensory bers derive from the C6 thumb emanate from the C6 DRG.27 Thus, the me-
DRG.27 Thus, based solely on anatomy, in addition to dian sensory NCS, recording from the thumb, as-
the LABC and musculocutaneous nerves, the LABC sesses the median nerve, lateral cord, upper trunk,
sensory NCS assesses the lateral cord, upper trunk, and the C6 anterior primary ramus, spinal nerve,
and the C6 anterior primary ramus, spinal nerve, and DRG (Fig. 5). Those bers innervating the in-
dex nger derive from the C6 and C7 DRG about
20% and 80% of the time, respectively.27 Hence, the
Table 2. CMAP domains of the brachial plexus elements.* median sensory NCS, recording from the index n-
ger, assesses the median nerve and lateral cord con-
Upper trunk Lateral cord
sistently; the upper trunk and the C6 anterior pri-
Musculocutaneous (biceps) Musculocutaneous (biceps)
Axillary (deltoid) mary ramus, spinal nerve, and DRG in 20% of
Middle trunk Posterior cord instances; and the middle trunk and the C7 anterior
Radial (anconeus) Axillary (deltoid) primary ramus, spinal nerve, and DRG in 80% of
Radial (extensor digitorum instances (Fig. 6). Those bers innervating the mid-
communis)
Radial (extensor indicis
proprius)
Radial (anconeus)
Lower trunk Medial cord
Ulnar (abductor digiti minimi) Ulnar (abductor digiti minimi)
Ulnar (rst dorsal Ulnar (rst dorsal
interosseous) interosseous)
Median (abductor pollicis Median (abductor pollicis
brevis) brevis)
Radial (extensor indicis
proprius)
CMAP, compound muscle action potential. FIGURE 4. Proposed brachial plexus pathway for the sensory
*The recording sites are shown in parentheses. bers assessed by the LABC SNAP.
Brachial Plexopathies MUSCLE & NERVE November 2004 553
Table 3. SNAP domains of the trunk and cord elements.*
Upper trunk Lateral cord
LABC (100%) LABC (100%)
Median (thumb) (100%) Median (thumb) (100%)
Supercial radial (60%) Median (index nger) (100%)
Median (index nger) (20%) Median (middle nger) (80%)
Median (middle nger) (10%)
Middle trunk Posterior cord
Median (index nger) (80%) Supercial radial (100%)
Median (middle nger) (70%) FIGURE 6. Proposed brachial plexus pathway for the sensory
Supercial radial (40%) bers assessed by the median SNAP recording from the index
Lower trunk Medial cord nger.
Ulnar (little nger) (100%) Ulnar (little nger) (100%)
MABC (100%) MABC (100%)
Median (middle nger) (20%) Median (middle nger) (20%) abnormalities noted among patients with plexopa-
LABC, lateral antebrachial cutaneous; MABC, medial antebrachial
thies related to median sternotomy, the cell bodies
cutaneous; SNAP, sensory nerve action potential. of origin of the sensory bers assessed by the ulnar
*The percentages shown in parentheses represent the frequency with sensory NCS, recording from the little nger or
which the sensory nerve bers subserving the listed SNAPs traverse the
different trunk and cord elements. The recording sites are shown in from the dorsal aspect of the hand, as studied by the
parentheses. dorsal ulnar cutaneous (DUC) nerveare primarily
located in the C8 DRG.27,84,96 Thus, these SNAPs
always depend on the integrity of the ulnar nerve,
dle nger arise from the C6, C7, and C8 DRG about medial cord, lower trunk, and the C8 anterior pri-
10%, 70%, and 20% of the time, respectively.27 Thus, mary ramus, spinal nerve, and DRG (Fig. 9). Based
the median sensory NCS, recording from this nger, on SNAP abnormalities noted among patients with
assesses the lateral cord in about 80% of instances true neurogenic TOS, as well as cadaver dissections,
and the medial cord in about 20% of instances. More the cell bodies of origin of the sensory bers assessed
proximally, it assesses the upper trunk and the C6 by the MABC sensory NCS reside predominantly in
anterior primary ramus, spinal nerve, and DRG in the T1 DRG.27,37,84,96,117,138 Thus, this study assesses
10% of instances; the middle trunk and the C7 an- the MABC nerve, medial cord, lower trunk, and the
terior primary ramus, spinal nerve, and DRG in 70% T1 anterior primary ramus, spinal nerve, and DRG
of instances; and the lower trunk and the C8 anterior (Fig. 10). The incidence of SNAP abnormalities as-
primary ramus, spinal nerve, and DRG in 20% of sociated with individual trunk and cord lesions is
instances (Fig. 7). shown in Table 3.
The cell bodies of origin of the sensory nerve
bers assessed by the supercial radial sensory NCS Electrodiagnostic Assessment of Individual Regions.
reside in the C6 and C7 DRG about 60% and 40% of Typically, lesions involving the brachial plexus do
instances, respectively.27 Thus, this study assesses the not affect all of its elements (i.e., they are regional)
supercial radial nerve, radial nerve, and posterior and, consequently, the entire plexus does not re-
cord consistently; the upper trunk and the C6 ante- quire exhaustive electrodiagnostic testing. Regard-
rior primary ramus, spinal nerve, and DRG in about ing the NCS, one approach is to screen the brachial
60% of instances; and the middle trunk and the C7 plexus using just ve sensory NCS (LABC; median
anterior primary ramus, spinal nerve, and DRG in recording from the thumb and index ngers; super-
about 40% of instances (Fig. 8). Based on SNAP
FIGURE 7. Proposed brachial plexus pathway for the sensory
FIGURE 5. Proposed brachial plexus pathway for the sensory bers assessed by the median SNAP recording from the middle
bers assessed by the median SNAP recording from the thumb. nger.
554 Brachial Plexopathies MUSCLE & NERVE November 2004
FIGURE 8. Proposed brachial plexus pathway for the sensory FIGURE 9. Proposed brachial plexus pathways for the sensory
bers assessed by the supercial radial SNAP. bers assessed by the ulnar SNAP recording from the little nger.
cial radial; and ulnar, recording from the little motor NCS, recording from extensor digitorum
nger). Whenever a specic region of the brachial communis (EDC) or anconeus, can be added,
plexus requires assessment, additional sensory NCS, though neither assesses solely the middle plexus.
motor NCS, and NEE of muscles belonging to that NEE of selected muscles (Table 4) is useful. Since
particular region are added (see Tables 4 and 5). isolated middle plexopathies are rare,1,27,75 their
Electrodiagnostic Assessment of the Supraclavicular identication should always prompt screening of the
Plexus. Upper plexus. The upper plexus contains adjacent upper and lower plexuses.
nerve bers from C5 and C6. Table 4 details its Lower plexus. The lower plexus (Table 4) con-
electrodiagnostic assessment. Regarding the sensory tains bers from C8 and T1. The ulnar sensory NCS,
NCS, although no studies assess the C5 DRG or its recording from the little nger, assesses the C8 DRG,
postganglionic bers, the other elements of the up- its postganglionic bers, and the lower trunk. The
per plexus are assessable. The median NCS, record- MABC study assesses the corresponding T1 struc-
ing from the thumb, and the LABC NCS both reli- tures. Thus, these two studies are complementary at
ably assess the C6 DRG, its postganglionic bers, and the pre-trunk level. Typically, with lower-trunk le-
the upper trunk. In general, upper plexopathies sions, both are equally affected, whereas their in-
tend to affect these two studies equally. These studies volvement is more discordant with more proximally
may need to be performed contralaterally to identify situated lesions. The DUC sensory NCS typically is
relative abnormalities (i.e., side-to-side differences superuous, since it assesses the same brachial
exceeding 50%). The supercial radial NCS and the plexus elements as the ulnar study.27 The ulnar [re-
median NCS, recording from the index nger, also cording from the abductor digiti minimi (ADM)]
assess these upper-plexus elements, albeit less reli- and median [recording from the abductor pollicis
ably (i.e., in 60% and 20% of instances, respec- brevis (APB)] motor NCS assess the lower plexus, as
tively).27 The musculocutaneous (recording biceps) does the radial motor NCS [recording from the
and axillary (recording deltoid) motor NCS assess all extensor indicis proprius (EIP)]. Although the latter
of the upper-plexus elements. To avoid relative ab- may be spared with partial lower-trunk lesions, its
normalities, these studies are performed bilaterally involvement excludes a medial cord lesion. These
in the presence of upper-plexus SNAP abnormalities three motor NCS assess the pre-trunk level of the
or whenever the recorded CMAP values are near or lower plexus differentiallythe radial NCS assesses
below their lower limit of normal. NEE of the shoul- solely the C8 root; the ulnar, the C8 root predomi-
der girdle, C5,6 radial, C5,6 axillary, and C6 me- nantly; and the median, almost solely the T1
dian innervated muscles is helpful, and evaluation of
levator scapulae, rhomboids, serratus anterior, and
spinati muscles helps to dene the proximal extent
of the lesion.
Middle plexus. The middle plexus (Table 4) con-
tains nerve bers from C7. The sensory nerve bers
subserving the median NCS, recording from the in-
dex and middle ngers, traverse the middle plexus
in approximately 80% and 70% of instances, respec-
tively; whereas those subserving the supercial radial
NCS traverse it in 40% of instances.27 Contralateral FIGURE 10. Proposed brachial plexus pathway for the sensory
studies help identify relative abnormalities. A radial bers assessed by the MABC SNAP.
Brachial Plexopathies MUSCLE & NERVE November 2004 555
Table 4. Electrodiagnostic assessment of the
affect these four SNAPs, only about 1 in 50 (2%)
supraclavicular plexus.* simultaneously involves all four studies and, when
this occurs, their degree of involvement tends to be
Upper plexus
Sensory NCS Needle electrode examination dissimilarthe median recording from the thumb
LABC Spinati muscles and LABC SNAPs are affected to a greater extent
Median (thumb) Deltoid than the median SNAPs recorded from the index
Supercial radial Biceps and middle ngers.27 On motor NCS, the musculo-
Median (index nger) Brachioradialis
cutaneous CMAP may be abnormal, but the axillary
Pronator teres
Motor NCS Extensor carpi radialis CMAP is spared. On NEE, abnormalities are re-
Axillary (deltoid) Triceps (lateral head) stricted to muscles innervated via musculocutaneous
Musculocutaneous (biceps) and C6,7median nerve bers. Muscles innervated
Radial (extensor digitorum by C5,6 radial and axillary nerve bers and by
communis or anconeus)
nerve derived from the anterior primary rami (long
Middle plexus
Sensory NCS Needle electrode examination thoracic and dorsal scapular nerves) and upper
Median (index nger) Triceps (lateral head) trunk (suprascapular nerve) help to differentiate an
Median (middle nger) Anconeus upper plexopathy.
Supercial radial Pronator teres Posterior cord. The only sensory NCS assessing
Flexor carpi radialis
this element is the supercial radial NCS (Table 5).
Motor NCS
Radial (anconeus) On motor NCS, the axillary CMAP and one of the
Lower plexus radial CMAPs are recorded. On NEE, muscles inner-
Sensory NCS Needle electrode examination
Ulnar (little nger) Abductor pollicis brevis
Dorsal ulnar cutaneous Flexor pollicis longus
Table 5. Electrodiagnostic assessment of the cords.*
MABC First dorsal interosseous
Ulnar (ring nger) Adductor pollicis Lateral cord
Abductor digiti minimi Sensory NCS Needle electrode examination
Motor NCS Flexor carpi ulnaris LABC Biceps
Ulnar (abductor digiti minimi) Flexor digitorum profundus Median (thumb) Brachialis
Ulnar (rst dorsal interosseous) 4,5 Median (index nger) Pronator teres
Median (abductor pollicis Extensor indicis proprius Median (middle nger) Flexor carpi radialis
brevis) Extensor pollicis brevis Motor NCS
Radial (extensor indicis Musculocutaneous (biceps)
proprius) Posterior cord
Sensory NCS Needle electrode examination
LABC, lateral antebrachial cutaneous; MABC, medial antebrachial Supercial radial Deltoid
cutaneous; NCS, nerve conduction study.
Motor NCS Triceps (lateral head)
*The entire muscle domain of the individual supraclavicular plexus regions is
not shown; only those muscles considered most helpful are included. Other Axillary (deltoid) Anconeus
helpful upper-plexus muscles include the serratus anterior, rhomboids, Radial (extensor digitorum Brachioradialis
teres minor, brachialis, exor carpi radialis, and, to a lesser degree, communis) Extensor carpi radialis
pectoralis major and levator scapulae. Other helpful middle-plexus muscles Radial (extensor indicis Extensor digitorum communis
include the extensor digitorum communis, extensor carpi ulnaris, and proprius) Extensor indicis proprius
extensor carpi radialis; lower-plexus muscles include the extensor carpi
ulnaris, extensor digitorum communis, pronator quadratus, and pectoralis
Radial (anconeus) Extensor pollicis brevis
minor. The recording sites are shown in parentheses. Medial cord
Sensory NCS Needle electrode examination
Ulnar (little nger) Abductor pollicis brevis
Dorsal ulnar cutaneous Flexor pollicis longus
root.27,78 Although the ulnar-elicited CMAP from the
MABC First dorsal interosseous
rst dorsal interosseous (FDI) reects the same Ulnar (ring nger) Adductor pollicis
lower-plexus elements as that from ADM, lower plex- Motor NCS Abductor digiti minimi
opathies may affect these two CMAPs differently and, Ulnar (abductor digiti minimi) Flexor digitorum profundus 4,5
thus, both often are required. With lower-plexus Ulnar (rst dorsal Flexor carpi ulnaris
interosseous)
SNAP abnormalities, CMAPs should be recorded bi-
Median (abductor pollicis
laterally. On NEE, it is useful to study muscles inner- brevis)
vated via C8,T1median, C8,T1 ulnar, and C8 ra-
dial motor nerve bers. LABC, lateral antebrachial cutaneous; MABC, medial antebrachial
cutaneous; NCS, nerve conduction study.
Electrodiagnostic Assessment of the Infraclavicular *The muscle domains of the posterior and medial cords are not shown in
Plexus. Lateral cord. Typically, lateral cord lesions their entirety. Rather, only those muscles considered most helpful are listed.
Other helpful posterior-cord muscles include the latissimus dorsi, extensor
affect the three median and LABC SNAPs uniformly carpi ulnaris, and teres minor. The pronator quadratus is a useful assessor
(Table 5). Although upper-trunk lesions may also of the medial cord. The recording sites are shown in parentheses.
556 Brachial Plexopathies MUSCLE & NERVE November 2004
vated via axillary, radial, and thoracodorsal nerve patients with ail arms, 75 were due to diffuse supra-
bers are helpful. To differentiate a middle plexus clavicular lesions; only 3 reected a diffuse infracla-
lesion, median SNAPs from the index and middle vicular plexopathy.5
ngers and NEE of muscles innervated via C6,7
median nerve bers are included. SELECTED SITE-SPECIFIC DISORDERS OF THE
Medial cord. Ulnar and MABC SNAPs and ulnar BRACHIAL PLEXUS
and median CMAPs are recorded (Table 5). The
Supraclavicular Plexopathies with Regional Predilec-
radial CMAP, recording from the EIP, is used to
tions. Upper Plexus. The most commonly injured
screen for a more proximal process. NEE of muscles
brachial plexus region is the upper plexus, usually
innervated via C8,T1median and C8,T1 ulnar
from closed traction.144,150 Brachial plexopathies
nerve bers is helpful. To screen for a more proxi-
with a predilection for the upper plexus include
mal process, muscles innervated via C8 radial nerve
bers [EIP; extensor pollicis brevis (EPB)] are burner syndrome, rucksack paralysis, and classic
added. Importantly, their normalcy does not exclude postoperative paralysis.
a more proximal process, as partial lower-trunk le- Burner syndrome. When sudden, forceful shoul-
sions may spare them. der contact produces separation of the shoulder and
Terminal nerves. Reliable sensory and motor head, upper plexus traction may occur; if associated
NCS are available to assess the median, radial, ulnar, with pain and paresthesias, the term burner or stinger
musculocutaneous, and axillary nerves. On NEE, is applied. As expected, these injuries are more com-
muscles innervated by these nerves are sampled. The mon among males involved in contact sports and are
lack of proximal branches emanating from these the most common of all sports-related injuries. In
terminal nerves means that it is impossible, by clini- one report, they accounted for 38% of 190 sports-
cal or electrodiagnostic means, to differentiate a related injuries.69 In general, the pain is abrupt in
terminal nerve lesion of the brachial plexus from a onset, sharp and burning in quality, and, with the
more distal, proximally located peripheral nerve le- paresthesias, extends distally into the upper extrem-
sion. ity, often to the thumb. These symptoms usually
Concluding Remarks. Typically, the ve screen- persist for a few minutes, longer in the presence of
ing sensory NCS listed in the introduction to this weakness. Their distribution implicates the C6 nerve
section are generally required, with additional stud- bers, but whether they are affected at a pre- or
ies based on the particular region under study or on postganglionic level is debated. Although some play-
any identied SNAP abnormalities. Patients with a ers experience numerous burners, permanent neu-
ail arm due to diffuse involvement of the distal rologic dysfunction is rare. Whenever the symptoms
supraclavicular plexus (pan-trunk plexopathy) or are prolonged, electrodiagnostic assessment is indi-
diffuse involvement of the proximal infraclavicular cated. With burners, the electrodiagnostic abnormal-
plexus (pan-cord plexopathy) can be difcult to dif- ities, when present, typically are limited to sparse
ferentiate by electrodiagnostic studies. Regarding brillation potentials in an upper-plexus distribu-
the sensory and motor NCS, only an abnormal su- tion.
prascapular motor NCS can identify a diffuse supra- Rucksack paralysis (cadet palsy; pack palsy). This
clavicular plexopathy. When normal, this study does typically unilateral upper plexopathy usually pre-
not distinguish a distal supraclavicular plexus lesion sents with painless weakness following or during the
(since the suprascapular nerve leaves the upper course of wearing a rucksack or similar device (e.g.,
trunk proximally) from a diffuse infraclavicular one. backpack, child-carrying harness). Sensory involve-
Although NEE of the muscles innervated by the ment, in the same distribution, often is present. Its
dorsal scapular, long thoracic, and suprascapular pathogenesis is likely nerve ber compression re-
nerves can be helpful, when normal the same distal lated to direct pressure from the rucksack. Risk fac-
pan-trunk versus pan-cord localization dilemma re- tors include the weight of the load transported, char-
mains. In this setting, examination of the pectoralis acteristics of the device itself (i.e., the presence of a
major muscle can be helpful, since it receives its metal frame or waist belt), and the duration worn.20
innervation via motor nerve bers exiting from the It may be more common in the presence of an
infraclavicular plexus so proximally that it tends to underlying abnormality (e.g., vertebral anomaly, cer-
be affected by supraclavicular plexopathies and vical rib) or previous local injury.155 A history of
spared by infraclavicular ones. Clinically, diffuse su- transient weakness following rucksack usage may be
praclavicular plexopathies are much more common elicited.144 In two-thirds of patients, the lesions are
than diffuse infraclavicular ones. In one report of 78 predominantly demyelinating conduction block.144
Brachial Plexopathies MUSCLE & NERVE November 2004 557
In this setting, the sensory NCS are normal and per plexopathies.29 Disorders with a predilection for
lesion localization and severity are determined by the lower plexus include true neurogenic TOS, fol-
the motor NCS and NEE. As expected with a demy- lowing surgery for disputed neurogenic TOS, post-
elinating process, treatment is conservative and re- median sternotomy brachial plexopathy, and Pan-
covery occurs within a few months. In the one-third coast syndrome. The percentage of closed traction
in whom axon loss predominates, recovery is more injuries involving the lower plexus is less than with
prolonged and may be incomplete. upper and middle plexopathies.150 Avulsion injuries
Classic postoperative paralysis. Classic postopera- are more common in this region of the supraclavic-
tive paralysis, which was initially described in 1894, is ular plexus.
a traction or pressure injury that characteristically True neurogenic thoracic outlet syndrome. The bra-
presents in the immediate postoperative setting as a chial plexus and subclavian vessels traverse the tho-
unilateral upper plexopathy or, much less fre- racic inlet, which lies between the rst rib and clav-
quently, as a more diffuse supraclavicular plexopathy icle and is commonly referred to as the thoracic
that involves the upper plexus disproportionately.144 outlet. When one of these structures is compressed
When involved, the middle and lower plexuses re- in that space, the general term TOS is applied. More
cover quicker, leaving an isolated upper plexopathy. specic terms include arterial TOS, venous TOS,
Clinically, the primary complaint is painless weak- and neurogenic TOS. The latter is divided into true
ness; paresthesias also may be noted. This entity is neurogenic and disputed neurogenic TOS. True
related to multiple factors, including patient posi- neurogenic TOS, which is more common among
tioning, loss of muscle tone from anesthesia, and younger women and has an incidence of approxi-
unconsciousness, which blocks weight-shifting abil- mately 1 per million, is also called the cervical rib
ity. Predisposing factors include the Trendelenburg and band syndrome because the affected C8 and T1
position; upper-extremity abduction beyond 90 de- bers of the lower plexus are stretched and angu-
grees; arm board restraint in an abducted, extended, lated by a taut band that extends from a rudimentary
and externally rotated position; and contralateral cervical rib or elongated C7 transverse process to the
deviation and rotation of the head.146 There is no rst rib.37 Since the T1 bers lie below the C8 bers,
gender or age group susceptibility. The underlying they are deected to a greater extent and, conse-
pathophysiology typically is demyelinating conduc- quently, sustain greater injury.37,38 This has both
tion block; much less frequently, axon loss predom- clinical and electrodiagnostic ramications. Clini-
inates.144,146 Thus, SNAPs assessing the upper plexus cally, patients present with T1 more than C8 weak-
(Table 4) usually are normal unless there is concom- ness and thenar muscle wasting, as well as paresthe-
itant axon loss. CMAP amplitude discrepancies be- sias and pain along the medial aspects of the arm,
tween axillary (normal) and supraclavicular fossa forearm, and hand. Likewise, the MABC SNAP and
(absent or low amplitude) stimulation sites indicate median CMAP (i.e., studies that primarily assess T1
a demyelinating conduction-block along upper- bers) are more affected than the ulnar SNAP and
plexus bers (musculocutaneous, recording from bi- CMAPs (i.e., studies that primarily assess C8 bers).
ceps; radial, recording from brachioradialis). An ab- The NEE indicates a slowly progressive axon-loss
sent or low-amplitude axillary CMAP is seen with process with a lower-plexus distribution that is most
supraclavicular fossa stimulation but, since this nerve pronounced in the APB muscle. This pattern of
cannot be stimulated infraclavicularly, an amplitude clinical and electrodiagnostic abnormalities is essen-
discrepancy cannot be sought. With demyelinating tially pathognomonic for true neurogenic TOS.27
conduction block lesions, rapid and full recovery is Although radiographic studies visualize associated
expected and, thus, conservative treatment is em- bony changes, they do not visualize the band. Surgi-
ployed.144,146,150 cal division of the band typically relieves the pain
Middle Plexus. Isolated middle plexopathies are and paresthesias and arrests the muscle weakness
rare.1,27,75 In one review of 417 brachial plexopa- and wasting.38,150 A single case with manifestations
thies, only one (surgically veried) was noted.27 similar to true neurogenic TOS was reported in a
More typically, middle-plexus involvement occurs competitive swimmer in whom the lower trunk was
with concomitant upper or lower plexus involve- compressed by a brous band located within a hy-
ment. Similar to upper plexopathies, the most com- pertrophied scalene muscle.59
mon cause of middle plexopathies is closed trac- Unlike true neurogenic TOS, which has a clear
tion.144 pathogenesis, objective clinical and electrodiagnos-
Lower Plexus. Among supraclavicular plexopa- tic features, and a good response to surgical inter-
thies, lower plexopathies are less common than up- vention, disputed neurogenic TOS has an unclear
558 Brachial Plexopathies MUSCLE & NERVE November 2004
pathogenesis, lacks objective clinical and electrodi- medial cord process, since lesions at these two sites
agnostic features, and does not reliably respond to tend to affect these two SNAPS more uniformly.) On
surgical intervention.143 Although some of its propo- motor NCS, isolated ulnar CMAP abnormalities may
nents believe that disputed neurogenic TOS is a be seen, accompanied infrequently by radial or me-
common and underdiagnosed disorder,109,110 many dian CMAP abnormalities (recording from EIP and
physicians do not even consider it a distinct entity. APB, respectively). Thus, localization typically rests
Oddly, among 174 patients in Colorado undergoing on the NEE. When present, abnormalities in muscles
surgery for TOS in 1989, almost all of them had supplied by C8 median nerve bers indicate that
either private insurance or workers compensation; the lesion lies at or proximal to the medial cord,
Medicaid patients almost never underwent surgery.13 whereas abnormalities in muscles innervated by C8
Postoperative disputed neurogenic thoracic outlet syn- radial nerve bers place it at or proximal to the
drome. When patients with disputed neurogenic lower trunk. Unless signicant axon loss involves the
TOS are treated surgically, especially by transaxillary dominant hand or causalgic pain develops, perma-
rst rib resection, some develop severe brachial plex- nent disability is unexpected and, thus, conservative
opathies, a condition termed postoperative disputed treatment usually is employed.29,41,54,78,136,137,144,150
neurogenic TOS.142 Most of these are incomplete, Pancoast syndrome. Since only the pleura sepa-
axon-loss lower plexopathies, though more extensive rates the lung from the T1 anterior primary ramus
damage may occur. These patients often present and lower trunk, lung diseases may involve the lower
with severe causalgic hand pain and clinical decits plexus. In 1924, Pancoast described the direct exten-
in the distribution of the affected brachial plexus sion of cancer from the lung apex to the lower
elements. Although the pain may improve after plexus.98,99 This syndrome occurs in about 3% of
surgical repair of the surgically traumatized ele- lung cancer patients and, thus, is most frequently
ments, the hand weakness typically does not do observed among men with a heavy smoking histo-
so.14,66,81,141,142,146,147,150 ry.104 Pancoast syndrome may also be observed
Postmedian sternotomy plexopathy. This term ap- among patients with lower plexopathies related to
plies to brachial plexopathies following operations other tumors (both benign and malignant), tumor
requiring median sternotomy, the most common of recurrences, and infectious or inammatory disor-
which is coronary artery bypass surgery.72 The clini- ders.51,150 With lung cancer, shoulder-region pain
cal and electrodiagnostic manifestations of this type typically is the initial and most pronounced symp-
of plexopathy suggest C8 anterior primary ramus tom. It may reect pleural, rib, spinal column, or
involvement; less commonly, adjacent elements also brachial plexus involvement. Interscapular pain may
are affected. Postulated etiologies incriminate the be present when the cancer involves the posterior
rst thoracic rib. Either chest wall retraction (1) primary rami.51 The shoulder pain tends to be burn-
pushes the clavicle into the retroclavicular space, ing or boring in character, worse at night, and tends
rotating the rst rib into the C8 anterior primary to radiate along the medial aspect of the arm to the
ramus, or (2) fractures the rst rib and the fractured elbow, and, less commonly, to the 4th and 5th dig-
segment impinges upon the C8 anterior primary its.51 When present, clinical decits are in a lower
ramus.64,78,136 In either case, a lower-plexus traction plexus distribution. When the cancer involves the T1
injury results that, by clinical and electrodiagnostic root or the inferior cervical sympathetic ganglion, a
assessments, affects the C8 anterior primary ramus Horners syndrome may appear. Pancoast syndrome
disproportionately. Although this ramus contains is often the rst manifestation of the neoplasm, com-
motor bers destined for the median, radial, and monly a nonsmall cell carcinoma; early recognition
ulnar nerves, its sensory bers are destined solely for and treatment are associated with a higher cure
the ulnar nerve. Thus, the associated paresthesias rate.71 Electrodiagnostic studies can localize the pro-
suggest an ulnar neuropathy. Misdiagnosis is avoided cess, thereby directing imaging studies. With severe
by clinical assessment of muscles supplied by C8 pain, narcotics and radiation therapy may be re-
median nerve (e.g., exor pollicis longus) and C8 quired.68
radial nerve bers (e.g., EIP, EPB). On sensory NCS,
an absent or low-amplitude ulnar SNAP recording Other Supraclavicular Plexopathies. Avulsions. Root-
from the little nger and a normal MABC SNAP lets are not surrounded by connective tissue and,
usually are seen, implying an ulnar neuropathy or a hence, are easily avulsed from the spinal cord by
ganglionic or postganglionic C8 root lesion. (Al- stretch (traction). Since the torn roots cannot regen-
though a fascicular process cannot be excluded, the erate or be surgically repaired, avulsions represent
normal MABC SNAP argues against a lower trunk or the most serious complication of traction injuries.
Brachial Plexopathies MUSCLE & NERVE November 2004 559
The ventral roots are more easily avulsed because delivery, thereby prompting excessive lateral devia-
they are of lesser caliber, have thinner dural sacs, tion of the head and neck in order to free the
and are more dispersed along the spinal cord than shoulder.21,135 When this plexopathy follows a
the dorsal roots.124 Regarding the brachial plexus, breech delivery, the risk of avulsion (usually of the
the lower two roots more commonly avulse, whereas C5 and C6 roots; less frequently of the C5C7 roots)
the upper two roots more commonly rupture ex- and bilateral involvement (22% in one series) is
traforaminally. This reects anatomic differences in increased.36 The fact that this type of plexopathy also
their proximal anchorage sites, angles of exit from follows deliveries by cesarean section implies that it
the intervertebral foramina, and lengths. The C5T1 does not simply follow poorly performed deliver-
spinal nerves traverse grooves in their respective ies.36,57,58,133,135,146 Reported risk factors include in-
transverse processes that lie between the intertrans- fantile macrosomia (common with maternal diabe-
versalis muscles. Since the C5 and C6, and variably tes), short mothers, low or midforceps delivery,
the C7, spinal nerves are securely anchored by fascia vacuum extraction, second-stage labor exceeding 60
at this point, their anchorage sites are extraforami- min, passive head rotation with the shoulders xed,
nal, whereas the C8 and T1 spinal nerves are an- multiparity, ethnic background, and delivery of a
chored at the spinal cord.125 In addition, the oblique previous infant with an obstetric brachial plexopa-
course of the upper cervical roots makes them more thy; fetal growth restriction and prematurity are con-
likely to tear extraforaminally than to avulse, sidered protective.20,21,79,135,153 The incidence of this
whereas the short length of the T1 root renders it type of plexopathy ranges from 0.52.6 per 1,000
more susceptible to avulsion.1 Upper-extremity posi- full-term live births 135 and reportedly is declining.20
tion at the time the traction force is applied also Five patterns of nerve ber involvement have been
plays a role. The C5C6 bers are most susceptible described: (1) C5C6 (Erbs palsy; about 50%); (2)
with the upper extremity alongside the torso, the C7 C5C7 (Erbs-plus palsy; waiters tip position, with
bers when it is oriented parallel to the oor, and adduction and internal rotation of arm, extension
the C8 T1 bers when it is in an above-shoulder and pronation of forearm, and exion of wrists and
position. Strong enough traction forces avulse all ngers; about 35%); (3) C5T1 with some nger
roots, regardless of limb position. Ruptures may be exion sparing; (4) C5T1 with ail arm and Hor-
incomplete, with one or more fascicles remaining in ners syndrome; and (5) C8 T1 with isolated paral-
continuity. Approximately 15% of supraclavicular le- ysis of the hand and Horners syndrome (Klumpkes
sions are two-level processes (preganglionic and palsy; almost never seen).135 Concomitant postgan-
postganglionic), especially with upper cervical root glionic lesions are more common with injuries in-
involvement.1 Concomitant axillary, musculocutane- volving the C5C7 bers (anchored extraforami-
ous, and suprascapular nerve injuries may occur at nally), whereas avulsion is more common with
their anchorage sites (i.e., quadrangular space, cor- lesions involving the C8 T1 bers (spinal cord an-
acobrachialis, and suprascapular or spinoglenoid choring).119 Although obstetric brachial plexopathy
notch, respectively). When the entire upper extrem- was rst described in 1764, its management remains
ity is paralyzed, including the long thoracic, dorsal controversial.87 These lesions range from mixed de-
scapular, thoracodorsal, and pectoral nerveinner- myelination and axonal to pure axon loss (avulsion)
vated muscles, especially in the presence of a Hor- but, in general, are less severe than traction injuries
ners syndrome, complete avulsion is likely. Other occurring among adults. Although many reviews sug-
indicators of possible avulsion include bony injury, gest that some spontaneous recovery occurs in over
especially a transverse process fracture (spinal nerve 90% of instances, its natural history is unknown.135
anchorage site); long-tract signs (damage severe Two Swedish studies, in which surgical intervention
enough to injure the spinal cord); and severe burn- was not employed, reported that 20 to 25% of pa-
ing pain, with shooting pain in the anesthetic ar- tients are signicantly impaired in later life.3,116,135
ea.155 Although extraforaminal ruptures may be Unfortunately, neither clinical nor electrodiagnostic
amenable to surgical repair, root avulsions are not. assessments can unequivocally identify this latter
Moreover, most avulsion injuries are associated with group. Hence, watchful waiting for evidence of re-
severe pain (especially hand pain), the incidence of covery usually is employed, though the duration of
which increases with the number of avulsed nerve such an approach is controversial. Since surgical
roots.148 repair yields the best results when performed within
Obstetric Brachial Plexopathy. Obstetric brachial the 1st year, the observation period usually ranges
plexopathy follows a type of traction injury that typ- from 3 to 9 months, or slightly longer.119 During this
ically occurs when shoulder dystocia impedes vertex time, physical therapy is employed. As expected, the
560 Brachial Plexopathies MUSCLE & NERVE November 2004
prognosis for C8 T1 nerve ber involvement is poor radial, axillary, and musculocutaneous nerves are
due to the greater incidence of avulsion injury. affected less frequently. Reportedly, lesions located
within the compartment (e.g., hematomas, aneu-
Infraclavicular Plexopathies with Regional Predilec- rysms, pseudoaneurysms, and other lesions with
tions. Disorders of the infraclavicular plexus have mass effect) cause the intracompartmental pressure
much less regional proclivity. At the cord level, radi- to rise, thereby impeding nerve ber microcircula-
ation directed at the axillary lymph nodes (mostly tion and inducing clinical dysfunction. If the pres-
women with breast cancer) tends to involve the in- sure increment were uniform, it should affect intra-
fraclavicular plexus, especially the lateral cord, compartmental nerves uniformly, whereas with this
whereas midshaft clavicular fractures more com- syndrome, the median nerve is affected dispropor-
monly affect the medial cord.18,24,60,88 At the termi- tionately. However, compartment syndromes associ-
nal nerve level, the median terminal nerve charac- ated with fractures are associated with pressure gra-
teristically is rst and most affected with medial dients that are greatest near the fracture site,48 and
brachial fascial compartment syndrome, and the ra- nerves located near a hematoma may be exposed to
dial terminal nerve is more frequently affected with greater pressures.42 Regarding axillary arteriograms,
crutch palsies. Of the ve terminal nerves, the mus- since the median and ulnar nerves lie near the axil-
culocutaneous terminal nerve is more often affected lary artery at the point of cannulation,97 the occur-
by operative procedures to correct recurrent ante- rence of a hematoma involves these two nerves out of
rior shoulder dislocation or by other procedures proportion to more distant ones, and the high pres-
performed near the coracoid process.12,32,150 Gleno- sures associated with the hematoma may account for
humeral dislocations and proximal humeral frac- the high incidence of these neuropathies. Clinically,
tures most commonly involve the axillary terminal patients present with pain or paresthesias in the
nerve, because of the short distance between its an- distribution of the affected nerves, followed shortly
chorage site and its point of origin,76 yet the nerve thereafter by weakness in a similar or wider distribu-
involvement frequently goes unnoticed. In one elec- tion. Without prompt surgical intervention, the
trodiagnostic study, performed 6 weeks after disloca- likelihood of recovery is poor. Thus, these lesions
tion, 35 of 65 (55%) patients had axillary terminal must be recognized early and decompressed ur-
nerve involvement, 8 of whom had a normal clinical gently.40,115,118,120,132,145,157 A recent study reported
examination.128 Suprascapular neuropathies are less that complete recovery was 8.3 times more likely
frequent and, when present, often coexist with axil- when surgical exploration occurred within the rst
lary neuropathies; musculocutaneous neuropathies 4 h of symptom onset.15 Electrodiagnostic testing,
are least common.148 These traction injuries range although useful for localizing and characterizing
from focal demyelination to total axon loss (e.g., neuropathies resulting from this syndrome, has no
nerve rupture, avulsion from the brachial plexus). role in the acute setting.
Other Infraclavicular Plexopathies. Staal et al. rst
SELECTED SITE-NONSPECIFIC BRACHIAL
described medial brachial fascial compartment syn- PLEXOPATHIES
drome in 1966, and it has recently been re-
viewed.120,132 The medial brachial fascial compart- Neuralgic Amyotrophy (Parsonage-Turner Syndrome).
ment, which extends from the clavicle to the elbow Although many names have been coined for this
and houses the terminal nerves of the brachial disorder, the term neuralgic amyotrophy (NA) con-
plexus and the axillary vessels, is formed by the veys its two quintessential features and thus is pre-
medial intermuscular septum, medially, when it di- ferred. Since NA has a predilection for predomi-
vides into two fascial extensions that extend to the nantly motor nerves, especially more proximally
brachial fascia that surrounds the arm. The ve ter- located ones, it frequently involves the long thoracic,
minal nerves of the brachial plexus exit from this suprascapular, and axillary nerves. The anterior in-
compartment in the following order: musculocuta- terosseous and musculocutaneous nerves, and nerve
neous, axillary, radial, ulnar, and median. The me- branches to individual muscles (e.g., infraspinatus,
dian nerve, characteristically, is affected rst, most pronator teres) also are frequently affected. The
severely, and most often in isolation. Isolated ulnar phrenic and medullary cranial nerves (especially the
or radial neuropathies are rare, and other mono- spinal accessory), as well as individual nerve roots,
neuropathies have not been described.118,132 When may be involved.17,55,91,103,112 Proximally, the nerve
two nerves are involved, the median and ulnar bers have a somatotopic arrangement. Therefore,
nerves are the most common combination.132 The although NA most commonly presents as a mono-
Brachial Plexopathies MUSCLE & NERVE November 2004 561
neuropathy or a multiple mononeuropathy, this may the degree of connective tissue involvement, and is
sometimes reect a proximal lesion within the bra- best determined by serial clinical and electrodiag-
chial plexus.122 Within the brachial plexus, the up- nostic assessments. Analgesics, including narcotics,
per trunk is most commonly affected.23 When biceps may be required for the initial pain. At that time, a
weakness is associated with musculocutaneous short course of corticosteroids may be helpful.74
CMAP and LABC SNAP abnormalities and the me- With chronic pain, neuropathic pain medications
dian SNAP recorded from the thumb is normal, a (e.g., gabapentin, tricyclics) are added. Strengthen-
musculocutaneous neuropathy is more likely than an ing and stretching exercises are indicated. Unlike
upper plexopathy.27 Conversely, when abnormal sporadic NA, the extremely rare familial form, which
LABC and median (recording from the thumb) has been localized to chromosome 17, is associated
SNAPs are recorded and a median neuropathy is with dysmorphic features (e.g., hypotelorism, high-
excluded (by normal median SNAPs from the index arched palate, syndactyly) and commonly re-
and middle ngers and a normal median CMAP), an curs.19,134,140,152
upper plexopathy is more likely. Bilateral NA may be
simultaneous or sequential and either symmetric or Primary Neoplastic Brachial Plexopathies. Neoplastic
asymmetric. When it recurs in a previously affected brachial plexopathies can be divided into primary
limb, it may involve the same or different nerves.144,148 (of brachial plexus origin) or secondary (originating
Clinically, abrupt and excruciating shoulder or outside the plexus). Primary brachial plexus tumors
upper-extremity pain, often with a nocturnal onset, are rare and usually benign. Of these, nerve sheath
is the presenting feature. Most commonly, the pain tumors predominate. Most are solitary schwannomas
is located at the lateral aspect of the shoulder or in or neurobromas involving the upper or middle
the periscapular region, but its location varies with plexus, proximally.148 Solitary schwannomas are
the involved nerve and can be most pronounced at slow-growing, encapsulated tumors that, at the root
the shoulder (axillary nerve), scapula (suprascapular level, more commonly affect the sensory roots. When
nerve), lateral thorax (long thoracic), antecubital they grow through the neural foramen and expand
fossa (anterior interosseous nerve), or lateral arm at both ends, they appear dumbbell-shaped.43 Most
and forearm (musculocutaneous nerve). Although patients present with a painless mass and may have
the pain may extend proximally or distally, shoulder paresthesias, sometimes exacerbated by motion or
movement rather than neck movement intensies it. palpation. Motor symptoms follow ventral root or
When its nature is unrecognized, unnecessary pro- spinal cord compression. On MR imaging, these le-
cedures may be performed.6 The severe pain typi- sions appear elliptical or spherical, isointense to
cally abates after 710 days or is replaced by a more muscle on T1 and hyperintense on T2, brightly en-
persistent dull ache. At this point, true weakness hance, and are often associated with entering, exit-
becomes apparent, as may signicant muscle wast- ing, or displaced fascicles.80 Pathologically, they arise
ing. About 50% of affected individuals report ante- from a single fascicle (plexiform schwannomas arise
cedent events, such as recent infection, unaccus- from multiple fascicles) and are thickly encapsu-
tomed exertion, childbirth, trauma, or an invasive lated. Once enucleated, they seldom recur. Solitary
medical or dental procedure. Although this triad intraneural neurobromas are benign, slowly grow-
(antecedent event, severe pain, and weakness and ing, nonencapsulated tumors that originate from the
wasting) generally is observed, considerable individ- neural sheath. Following excision, recurrence is un-
ual variation exists.22 Sensory NCS help to localize usual, even when incomplete.43 When these tumors
the lesion. The motor NCS dene the severity of the occur as part of neurobromatosis type 1, they do
affected nerves and thus are useful as baseline prog- not have a regional predilection and more fre-
nosticators and for subsequent comparative mea- quently are multiple and plexiform, recur following
surements. Consistent with an axon-loss process, the excision, and, like malignant nerve sheath tumors,
NEE shows ndings indicative of acute and chronic present with pain or clinical decits.119,150 On MR
motor axon loss, the combination of which reects imaging, they appear fusiform or plexiform in shape,
the timing of the study.101,105,144 Rarely, early in its isointense to muscle on T1 and hyperintense on T2,
course, demyelinating conduction block may pre- and enhance. Unlike schwannomas, displaced fasci-
dominate, as evidenced by full and rapid recovery cles are rare.80
from severe weakness or by the electrodiagnostic Malignant nerve sheath tumors arise de novo or
study itself.139 Tsairis et al. reported recovery rates of via malignant transformation usually from a plexi-
36% by 1 year, 75% by 2 years, and 89% by 3 years.131 form neurobroma, less commonly from a solitary
Recovery reects lesion severity, lesion location, and intraneural neurobroma, and rarely from a schwan-
562 Brachial Plexopathies MUSCLE & NERVE November 2004
noma.100 Patients often present with painful, enlarg- the paresthesias and, later, weakness.151 Typically,
ing masses associated with appropriately distributed these lesions are relentlessly progressive.39 Because
clinical decits. Their highly malignant nature is the paresthesias involve the lateral digits, carpal tun-
reected by their 5-year survival rate (10 to 50%).100 nel syndrome may be suspected unless electrodiag-
On MR imaging, these tumors are less circumscribed nostic testing is performed. When related to radia-
and may be observed to extend along fascial tion, the initial electrodiagnostic manifestations
planes.80 Complementary studies include CT scans, typically include demyelinating conduction block on
angiograms, and myelograms.80,100 In the future, MR motor NCS, and myokymic discharges and fascicula-
neurography may be helpful in demonstrating these tion potentials on NEE.25,39,68,73 The paraspinal mus-
lesions.85 cles are studied, especially if tumor recurrence is
being considered, because paraspinal brillation po-
Secondary Neoplastic Brachial Plexopathies. Neo- tentials are more common with radiation therapy
plastic processes that involve the brachial plexus sec- than tumor recurrence.44 Unlike most demyelinat-
ondarily (usually breast or lung cancers) do so by ing conduction-block lesions, those associated with
means of extrinsic compression or inltration from radiation therapy are prolonged and typically con-
adjacent structures or spread from distant sites (me- vert to axon loss, with electrodiagnostic features that
tastases). When cancer involves the axillary lymph reect the timing of the study and the severity of the
nodes, it may inltrate the medial cord or nearby loss. As axon loss progresses, the limb eventually
nerves (medial brachial cutaneous, MABC, ulnar, or becomes nonfunctional, accounting for the dismal
median). Most patients present with severe and per- prognosis of these lesions.151 The delayed effects of
sistent shoulder and upper-extremity pain, followed radiation therapy likely reect ischemic damage re-
by appropriate clinical decits. With sympathetic in- lated to microcirculatory impairment from radia-
volvement, the upper extremity may become warm tion-induced brosis.20 Rarely, radiation therapy
and dry and a Horners syndrome sometimes devel- generates nerve sheath tumors, typically malignant
ops. With spread throughout the brachial plexus, ones.33
symptom distribution increases.68,71,104 Although It is important to distinguish neoplastic from
plain lms, bone scans, and CT-myelography (when radiation-induced plexopathy. Clinically, with neo-
epidural metastases are present) may demonstrate plastic plexopathies, the incidence of pain at onset
evidence of malignancy or metastatic disease, MR and Horners syndrome is much higher, whereas
imaging is the radiographic procedure of choice for with radiation plexopathies, isolated paresthesias
evaluating neoplastic plexopathies. Through lesion predominate.44,68,73 Although the electrodiagnostic
localization, electrodiagnostic testing can direct abnormalities typical of radiation therapy may be
these studies. Since neoplastic processes frequently observed, their presence does not exclude concom-
invade the brachial plexus from below, electrodiag- itant tumor recurrence. On MR imaging, nodular
nostic assessment of T1 bers is mandatory. Initially, enhancement is highly suggestive of a neoplastic
MABC SNAP abnormalities may be the only electro- process,100 as is the presence of a mass.127 Unfortu-
diagnostic manifestation of T1 sensory ber inltra- nately, even surgical exploration with biopsy may be
tion.114 nondiagnostic.68,73 In the future, it may be possible
to differentiate recurrent cancer from radiation
Radiation-Induced Brachial Plexopathy. Although changes using MR neurography.31,85 Reversible bra-
the PNS is relatively resistant to radiation damage, chial plexopathies also follow radiation therapy.111
the incidence of damage increases with higher total Although there is no effective treatment for plexopa-
dose, larger fraction sizes, and application times of thies following radiation, neurolysis may ameliorate
shorter duration. Thus, lower doses administered severe pain, when present, although this may result
over longer periods are safer.43,77,123,155 The rst in greater clinical decits.66,144,148
cases of radiation-induced brachial plexopathy were
reported in 1964.92 These plexopathies are more Traumatic Brachial Plexopathies. These typically re-
often observed among women with breast cancer sult from closed traction, most of which follow high-
who received axillary lymph node chain radiation velocity injuries (e.g., motor vehicle accidents, espe-
therapy months to decades earlier.126 Radiation- cially those involving motorcycles), or sports and
induced brachial plexopathies typically are painless occupational injuries. Most closed-traction injuries
lesions that usually present with paresthesias involv- produce supraclavicular plexopathies, typically up-
ing one or more of the lateral three digits (i.e., per plexopathies that follow elongation of the bra-
lateral cord distribution), followed by extension of chial plexus by forceful separation of the head and
Brachial Plexopathies MUSCLE & NERVE November 2004 563
shoulder.34,89,90 Lower-plexus traction injuries are include worsening pain or neurologic dysfunction,
less common and usually follow forceful separation hematoma formation, concomitant bone or vascular
of the upper extremity from the torso. Traction in- injuries, and compartment syndrome.119 With blunt
juries involving the infraclavicular plexus, as with lacerations, repair is delayed until the proximal and
infraclavicular plexopathies in general, more com- distal extents of the neuroma are appreciable.66,119
monly are associated with bone and blood vessel Since the affected brachial plexus elements injured
injury.65 Open traction injuries are less common and by high-velocity rounds are infrequently disrupted,
usually result from gunshot or chainsaw accidents.148 these lesions usually are initially (2 4 months) man-
Penetrating injuries most commonly involve the in- aged conservatively, with surgical intervention being
fraclavicular plexus. Low-velocity insults (e.g., knife employed for those individuals not showing im-
blade, low-velocity round) produce damage by direct provement. Resection with graft placement usually is
contact, unless the injury occurs in a delayed man- required.66
ner (e.g., hematoma or pseudoaneurysm formation
following vessel injury).66,148 The pressure waves and Iatrogenic Brachial Plexopathy. Iatrogenic brachial
cavitation created by the passage of a high-velocity plexopathies constitute about 7 to 10% of brachial
round can indirectly damage the brachial plexus by plexopathies, the majority of which are blunt lesions
contusive and traction forces related to the cube of in continuity.66,67,94,146 Most follow operations and
its velocity.8,10,66 Although these forces infrequently other medical procedures and are related to a num-
disrupt the brachial plexus, they may be quite ber of factors, including patient position (e.g., classic
lengthy.66 Transecting injuries may be either sharp postoperative paralysis) and the particular proce-
(knives, glass) or blunt (metal fragments, fan or dure performed (e.g., median sternotomy). Some
motor blades, chain saws, animal bites). Compres- iatrogenic brachial plexopathies have predisposi-
sion injuries usually occur between the clavicle and tions for particular brachial plexus regions or ele-
rst rib. Since the clavicle overlies the divisions, ments, as discussed earlier. The frequent location of
these injuries tend to involve the distal trunk, divi- the musculocutaneous nerve within the so-called
sion, and proximal cord elements. In the com- conjoint tendon renders it susceptible to procedures
pressed state, contralateral head movement pro- performed in this area.12,32,53 Like other traumatic
duces traction forces on the roots and trunks, plexopathies, iatrogenic brachial plexopathies may
whereas downward or lateral arm movement places affect the plexus directly (e.g., suture or hardware
traction forces on the cords. misplacement, element transection, injection injury)
The treatment of traumatic brachial plexopa- or indirectly (e.g., pseudoaneurysm or hematoma
thies reects the type of injury, its location, its sever- formation) and, hence, do not always present
ity, and its chronicity.119 Most closed injuries are acutely. With midshaft clavicular fractures, the
associated with lesions in continuity and are treated plexus can be acutely damaged by sharp bony edges
conservatively since it is impossible at that time to or subsequently damaged by hypertrophic callus,
determine the likelihood of recovery or the type of nonunion, or a subclavian pseudoaneurysm.4,18,22
surgical repair necessary.119 Conservative manage- When surgically placed screws subsequently loosen,
ment includes physical therapy, and serial clinical detach, and damage nearby vascular structures, pro-
and electrodiagnostic assessments. When patients ducing a hematoma or pseudoaneurysm, the plexus
with focal lesions show no signs of recovery after 23 injury can develop long after screw place-
months (4 5 months for lengthier lesions), they are ment.26,106,146 Treatment, like that of other traumatic
candidates for surgical exploration.119 Shorter obser- brachial plexopathies, reects the type of injury and
vation periods (3 weeks to 3 months) may be con- its location, severity, and chronicity. With misplaced
sidered for high-energy injuries or those associated sutures or hardware, the offending item is removed
with total or near-total paralysis.49 Most infraclavicu- and the element repaired; with sharp transections,
lar plexopathies following humeral fracture or gle- acute end-to-end repair typically is employed; and
nohumeral dislocation (mostly axillary neuropa- with blunt transections, treatment usually is delayed
thies) are treated conservatively, unless a severe long enough to permit neuroma formation.66 Inju-
lesion in continuity or a rupture is present.150 Sharp ries related to malpositioning or following proce-
lacerations usually are repaired acutely (within dures involving sternal splitting typically are treated
72 h), by primary end-to-end neurorrhaphy, because conservatively. With sharp injuries, surgical repair
they are easier to assess prior to the onset of scarring typically is performed within the rst 72 h, whereas
and because their length is not lost to retrac- with blunt injuries, it typically is delayed for several
tion.49,66,119 Other indications for acute intervention weeks.66
564 Brachial Plexopathies MUSCLE & NERVE November 2004
PROGNOSIS
REFERENCES
The prognosis for a brachial plexus injury reects
1. Alnot JY. Traumatic paralysis of the brachial plexus: preop-
lesion localization and severity. Disorders producing erative problems and therapeutic indications. In: Terzis JK,
isolated demyelination recover following remyelina- editor. Microreconstruction of nerve injuries. Philadelphia:
tion, a process that typically occurs within 2 to 8 WB Saunders; 1987. p 325346.
2. Armington WG, Harnsberger HR, Osborn AG, Seay AR.
weeks. However, in certain settings, demyelination Radiographic evaluation of brachial plexopathy. AJNR 1987;
more commonly converts to axon loss (e.g., radia- 8:361367.
tion plexopathies) or is prolonged and frequently 3. Bager B. Perinatally acquired brachial plexus palsy: a persist-
ing challenge. Acta Paediatr 1997;86:1214 1219.
unresponsive to therapy (e.g., multifocal motor neu- 4. Barbier O, Malghem J, Delaere O, Vande Berg B, Rombouts
ropathy). The majority of brachial plexopathies are JJ. Injury to the brachial plexus by a fragment of bone after
related to isolated axon loss and the prognosis for fracture of the clavicle. J Bone Joint Surg 1997;79B:534 536.
5. Bentolila V, Nizard R, Bizot P, Sedel L. Complete traumatic
their recovery reects their potential for reinnerva- brachial plexus palsy. Treatment and outcome after repair.
tion, which in turn reects lesion completeness and J Bone Joint Surg 1999;81A:20 28.
distance from the denervated muscle bers, as well 6. Beydoun SR, Rodriguez R. Neuralgic amyotrophy misdiag-
nosed as diaphragmatic rupture. Muscle Nerve 1996;19:1181
as the degree of associated connective tissue involve- 1182.
ment. Complete lesions are not amenable to rein- 7. Birch R, Bonney G, Wynn Parry CB. Surgical disorders of
nervation via collateral sprouting because the latter peripheral nerves. London: Churchill Livingstone; 1998.
539 p.
require unaffected nerve bers from which to 8. Black AN, Burns BD, Zuckerman S. An experimental study
sprout. Lesions located more than 20 24 inches of the wounding mechanism of high velocity missiles. BMJ
1941;2:872 874.
from the denervated muscle bers are not amenable
9. Bonnel F. Microscopic anatomy of the adult human brachial
to reinnervation via proximodistal axon advance- plexus: an anatomical and histological basis for microsur-
ment, which occurs at a rate of 1 inch per month, gery. Microsurgery 1984;5:107117.
10. Callender GR. Wound ballistics: mechanism of production
because muscle bers cannot survive in the dener- of wounds by small arms, bullets, and shell fragments. War
vated state for more than 20 to 24 months. Connec- Med 1943;3:337342.
tive tissue (endoneurium, perineurium, and 11. Carvalho GA, Nikkhah G, Matthies C, Penkert G, Sammi M.
Diagnosis of root avulsions in traumatic brachial plexus in-
epineurium) disruption at the lesion site leads to juries: value of computerized tomography myelography and
brosis, which impedes axon advancement.113,125 magnetic resonance imaging. J Neurosurg 1997;86:69 76.
Unfortunately, there are no electrodiagnostic mani- 12. Caspi I, Exra E, Nerubay J, Horoszovski H. Musculocutane-
ous nerve injury after coracoid process transfer for clavicular
festations by which to judge the degree of brotic stability. Acta Orthop Scand 1987;58:294 295.
impediment, and the only clinical manifestation is 13. Cherington M, Cherington C. Thoracic outlet syndrome:
the passage of time (i.e., failure to recover). reimbursement patterns and patient proles. Neurology
1992;42:943945.
Even when sensory and motor functions are re- 14. Cherington M, Happer I, Machanic B, Parry L. Surgery for
captured, persistent and unresponsive pain may oc- thoracic outlet syndrome may be hazardous to your health.
cur. Not infrequently, analgesics, neuropathic pain Muscle Nerve 1986;9:632 634.
15. Chitwood RW, Shepard AD, Shetty PC, Burke MW, Reddy
medications, transcutaneous electical nerve stimula- DJ, Nypaver TJ, Ernest CB. Surgical complications of transax-
tion (TENS) units, stellate ganglion blocks, dorsal illary arteriography: a case controlled study. J Vasc Surg
1996;23:844 850.
column stimulation, and various surgical procedures 16. Clemente CD. Grays Anatomy, 30th American ed. Philadel-
(e.g., neurolysis, sympathectomies, stellate gan- phia: Lea & Febiger; 1985. 1466 p.
glionectomies, amputation, cordotomies, and dorsal 17. Comroe JH, Wood FC, Kay CF, Spoont EM. Motor neuritis
after tetanus antitoxin with involvement of muscles of respi-
root entry zone ablations) are ineffective.148 ration. Am J Med 1951;10:786 789.
The operative outcomes associated with supracla- 18. Della Santa D, Narakas A, Bonnard C. Late lesions of the
vicular lesions typically are most favorable for upper brachial plexus after fracture of the clavicle. Ann Chir Main
Memb Super 1991;10:531540.
plexopathies (more likely extraforaminal; closer to 19. Dreschfeld J. On some of the rarer forms of muscular atro-
denervated organs), least favorable for lower plex- phies. Brain 1886;9:178 195.
opathies (more likely avulsion; further from dener- 20. Dumitru D, Zwarts MJ. Brachial plexopathies and proximal
mononeuropathies. In: Dumitru D, Amato AA, Zwarts MJ,
vated organs), and intermediate for mixed upper editors. Electrodiagnostic medicine, 2nd ed. Philadelphia:
and middle plexopathies. Regarding infraclavicular Hanley & Belfus; 2002. p 777 836.
processes, surgical outcomes are better for lateral 21. Eng GD, Binder H, Getson P, ODonnell R. Obstetrical
brachial plexus palsy (OBPP) outcome with conservative
and posterior cord repairs than for medial cord management. Muscle Nerve 1996;19:884 891.
repairs.66 22. England JD. The variations of neuralgic amyotrophy. Muscle
Nerve 1999;22:435 436.
The author thanks Asa J. Wilbourn, MD, for reviewing this manu- 23. England JD, Sumner AJ. Neuralgic amyotrophy: an increas-
script, his post-fellowship mentoring, and his friendship. ingly diverse entity. Muscle Nerve 1987;10:60 68.
Brachial Plexopathies MUSCLE & NERVE November 2004 565
24. England JD, Tiel RL. Costoclavicular mass syndrome. Muscle 47. Haymaker W, Woodhall B. Peripheral nerve injuries: princi-
Nerve 1999;22:412 418. ples of diagnosis. Philadelphia; WB Saunders; 1953. 333 p.
25. Esteban A, Traba A. Fasciculation-myokymic activity and pro- 48. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD.
longed nerve conduction block: a physiopathological rela- Compartment pressure in association with closed tibial frac-
tionship in radiation-induced brachial plexopathy. Electro- tures. J Bone Joint Surg 1994;76A:12851292.
encephalogr Clin Neurophysiol 1993;89:382391. 49. Hentz VR. Brachial plexus injuries. In: Omer GE Jr, Spinner
26. Fee HJ, McAvoy JM, Dainko EA. Pseudoaneurysms of the M, Van Beek AL, editors. Management of peripheral nerve
axillary artery following a modied Bristow operation: report problems, 2nd ed. Philadelphia: WB Saunders; 1998. p 445
of a case and review. J Cardovasc Surg 1978;19:65 68. 453.
27. Ferrante MA, Wilbourn AJ. The utility of various sensory 50. Hentz VR, Narakas AO. The results of microneurosurgical
nerve conduction responses in assessing brachial plexopa- reconstruction in complete brachial plexus palsy. Orthop
thies. Muscle Nerve 1995;18:879 889. Clin North Am 1988;19:107114.
28. Ferrante MA, Wilbourn AJ. Basic principles and practice of 51. Hepper NGG, Herskovic T, Witten DM, Mulder DW, Wool-
EMG. In: Younger DS, editor. Motor disorders. Philadelphia: ner LB. Thoracic inlet tumors. Ann Intern Med 1966;64:
Lippincott, Williams, & Wilkins; 1999. p 19 44. 979 989.
29. Ferrante MA, Wilbourn AJ. Plexopathies. In: Levin KH, Lud- 52. Hollinshead WH. Anatomy for surgeons, Vol 3: the back and
ers HO, editors. Comprehensive clinical neurophysiology. limbs, 3rd ed. Philadelphia: Harper & Row; 1982. 880 p.
Philadelphia: WB Saunders; 2000. p 201214. 53. Hoppenfeld S, deBoer P. Surgical exposures in orthopae-
30. Ferrante MA, Wilbourn AJ. Electrodiagnostic approach to dics: the anatomic approach. Philadelphia: Lippincott; 1984.
the patient with suspected brachial plexopathy. Neurol Clin p 1 45.
2002;20:423 450. 54. Hotson JR. Neurological sequelae of cardiac surgery. In:
31. Filler A. Imaging of peripheral nerve. In: Katirji B, Kaminski Aminoff MJ, editor. Neurology and general medicine. New
HJ, Preston DC, Ruff RL, Shapiro BE, editors. Neuromuscu- York: Churchill Livingstone; 1989. p 49 59.
lar disorders in clinical practice. Boston: Butterworth Hei- 55. James JL, Miles DW. Neuralgic amyotrophy: a clinical and
nemann; 2002. p 266 282. electromyographic study. BMJ 1966;2:10421043.
32. Flatow EL, Bigiani LU, April EW. An anatomic study of the 56. Jelasic F, Piepgrass U. Functional restitution after cervical
musculocutaneous nerve and its relationship to the coracoid avulsion injury with typical myelographic ndings. Eur
process. Clin Orthop 1989;244:166 171. J Neurol 1974;11:158 163.
33. Foley KM, Woodruff JM, Ellis FT, Posner JB. Radiation- 57. Jennett RJ, Tarby TJ. Brachial plexus palsy: an old problem
induced malignant and atypical peripheral nerve sheath revisited again. Am J Obstet Gynecol 1997;176:1354 1357.
tumors. Ann Neurol 1980;7:311318. 58. Jones HR Jr. Pediatric electromyography. In: Brown WF,
34. Frykholm R. The mechanism of cervical radicular lesions Bolton CF, editors. Clinical electromyography, 2nd ed. Bos-
resulting from stretch and forceful traction. Acta Chir Scand ton: Heinemann; 1993. p 695758.
1957;102:9396.
59. Katirji B, Hardy RW Jr. Classic neurogenic thoracic outlet
35. Fuller GN, Dick JPR, Colquhoun IR. Brachial plexus com-
syndrome in a competitive swimmer: a true scalenus anticus
pression by hematoma following jugular puncture. Neurol-
syndrome. Muscle Nerve 1995;18:229 233.
ogy 1994;44:775776.
60. Kay SP, Eckardt JJ. Brachial plexus palsy secondary to clavic-
36. Geutjens G, Gilbert A, Helsen K. Obstetric brachial plexus
ular nonunion. Clin Orthop 1986;206:219 222.
palsy associated with breech delivery: a different pattern of
61. Kendall FP, McCreary EK, Provance PG. Muscles. Testing
injury. J Bone Joint Surg [Br] 1996;78:303306.
and function, 4th ed. Baltimore: Williams & Wilkins; 1993. p
37. Gilliatt RW. Thoracic outlet syndromes. In: Dyck PJ, Thomas
406 407.
PK, Lambert EH, Bunge R, editors. Peripheral neuropathy,
2nd ed. Philadelphia: Saunders; 1984. p 1409 1424. 62. Kerr AT. The brachial plexus of nerves in man: the variations
38. Gilliatt RW, Le Quesne PM, Logue V, Sumner AJ. Wasting of in its formation and branches. Am J Anat 1918;23:285395.
the hand associated with a cervical rib or band. J Neurol 63. Kewalramani LS, Taylor RG. Brachial plexus root avulsion:
Neurosurg Psychiatry 1970;33:615 624. role of myelography. Review of diagnostic procedures.
39. Glantz MJ, Burger PC, Friedman AH, Radtke RA, Massey J Trauma 1975;15:603 608.
EW, Schold SC Jr. Treatment of radiation-induced nervous 64. Kirsh MM, Magee KR, Gago O, Kahn DR, Sloan H. Brachial
system injury with heparin and warfarin. Neurology 1994;44: plexus injury following median sternotomy incision. Ann
2020 2027. Thorac Surg 1971;11:315319.
40. Groh GI, Gainor BJ, Jeffries JT, Brown M, Eggers GW Jr. 65. Kline DG. Civilian gunshot wounds to the brachial plexus.
Pseudoaneurysms of the axillary artery with median nerve J Neurosurg 1989;70:166 174.
decit after axillary block anesthesia. J Bone Joint Surg 66. Kline DG, Hudson AR. Nerve injuries. Philadelphia: WB
1990;72A:14071408. Saunders; 1995. 611 p.
41. Hanson MR, Breuer AC, Furlan AJ, Lederman RJ, Wilbourn 67. Kline DG, Judice DJ. Operative management of selected
AJ, Cosgrove DM, Loop FD, Estafanous FG. Mechanism and brachial plexus lesions. J Neurosurg 1983;58:631 649.
frequency of brachial plexus injury in open-heart surgery: a 68. Kori SH, Foley KM, Posner JB. Brachial plexus lesions in
prospective analysis. Ann Thorac Surg 1983;36:675 679. patients with cancer: 100 cases. Neurology 1981;31:4550.
42. Hargens AR, Mubarak SJ. Current concepts in the patho- 69. Krivickas LS, Wilbourn AJ. Sports and peripheral nerve in-
physiology, evaluation, and diagnosis of compartment syn- juries: report of 190 injuries evaluated in a single electro-
drome. Hand Clin 1998;14:371383. myographic laboratory. Muscle Nerve 1998;21:10921094.
43. Harkin JC, Reed RJ. Tumors of the peripheral nervous sys- 70. Krudy AG. MR myelography using heavily T2-weighted fast
tem. Washington DC: Armed Forces Institute of Pathology; spin-echo pulse sequences with fat presaturation. AJR Am J
1969. 174 p. Roentgenol 1992;159:13151320.
44. Harper CM, Thomas JE, Cascino TL, Litchy WJ. Distinction 71. Layzer RB. Neuromuscular manifestations of systemic dis-
between neoplastic and radiation-induced brachial plexopa- ease. Philadelphia: FA Davis; 1985. 434 p.
thy, with emphasis on the role of EMG. Neurology 1989;39: 72. Lederman RJ, Breuer AC, Hanson MR, Furlan AJ, Loop FD,
502506. Cosgrove DM, Estafanous FG, Greenstreet RL. Peripheral
45. Harris W. Prexed and postxed types of brachial plexus. nervous system complications of coronary artery bypass graft
Brain 1903;26:613 615. surgery. Ann Neurol 1982;12:297301.
46. Harris W. The true form of the brachial plexus and its motor 73. Lederman RJ, Wilbourn AJ. Brachial plexopathy: recurrent
distribution. J Anat Physiol 1904;38:399 422. cancer or radiation? Neurology 1984;34:13311335.
566 Brachial Plexopathies MUSCLE & NERVE November 2004
74. Lederman RJ, Paulson SM. Brachial neuritis. In: Johnson 98. Pancoast HK. Importance of careful roentgen-ray investiga-
RT, editor. Current therapy in neurology, 2nd ed. Philadel- tions of apical chest tumors. JAMA 1924;83:1407.
phia: Decker; 1987. p 320 322. 99. Pancoast HK. Superior pulmonary sulcus tumor: tumor char-
75. Leffert RD. Brachial plexus injuries. New York: Churchill acterized by pain, Horners syndrome, destruction of bone
Livingstone; 1985. 243 p. and atrophy of hand muscles. JAMA 1932;99:13911396.
76. Leffert RD, Seddon HJ. Infraclavicular brachial plexus inju- 100. Park JK. Peripheral nerve tumors. In: Samuels MA, Feske SK,
ries. J Bone Joint Surg 1965;47B:9 23. editors. Ofce practice of neurology, 2nd ed. Philadelphia:
77. Leibel SA, Sheline GE. Tolerance of the central and periph- Churchill Livingstone; 2003. p 1118 1121.
eral nervous system to therapeutic irradiation. Adv Rad Biol 101. Parsonage MJ, Turner AJW. Neuralgic amyotrophy: the
1987;12:257288. shoulder girdle syndrome. Lancet 1948;1:973978.
78. Levin KH, Wilbourn AJ, Maggiano HJ. Cervical rib and 102. Perotto AO. Anatomical guide for the electromyographer:
median sternotomy-related brachial plexopathies: a reassess- the limbs and trunk, 3rd ed. Springeld: Thomas; 1994. p
ment. Neurology 1998;50:14071413. 305307.
79. Levine MG, Holroyde J, Woods JRJ, Siddiqi JA, Scott M, 103. Pierre PA, Laterre CE, Van Den Bergh PY. Neuralgic amy-
Miodovnik M. Birth trauma: incidence and predisposing otrophy with involvement of cranial nerves IX, X, XI, and
factors. Obstet Gynecol 1984;63:792795. XII. Muscle Nerve 1990;13:704 707.
80. Lin J, Martel W. Cross-sectional imaging of peripheral nerve 104. Posner JB. Neurologic complications of cancer. Philadel-
sheath tumors: characteristic signs on CT, MR imaging, and phia: FA Davis; 1995. 482 p.
sonography. AJR Am J Roentgenol 2001;176:75 82. 105. Rennels GD, Ochoa J. Neuralgic amyotrophy manifesting as
81. Lindgren K. Reasons for failures in surgical treatment of anterior interosseous nerve palsy. Muscle Nerve 1980;3:160
thoracic outlet syndrome. Muscle Nerve 1995;18:1484 1486. 164.
82. Liveson JA. Peripheral neurology: case studies in electrodi- 106. Richards RR, Hudson AR, Bertoia JT, Urbaniak JR, Waddell
agnosis, 2nd ed. Philadelphia: Davis; 1992. p 36 42. JP. Injury to the brachial plexus during Putti-Platt and Bris-
83. Liveson JA, Ma DM. Laboratory reference for clinical neu- tow procedures: a report of 8 cases. Am J Sports Med 1987;
rophysiology. Philadelphia: Davis; 1991. p 415 423. 15:374 380.
84. Maggiano H, Levin KH, Wilbourn AJ. Relationship between 107. Robles J. Brachial plexus avulsion: a review of diagnostic
the medial antebrachial cutaneous sensory and median mo- procedures and report of six cases. J Neurosurg 1947;28:
tor responses in brachial plexopathies. Muscle Nerve 1993; 434 438.
16:11131114. 108. Roger B, Travers V, Laval-Jeantet M. Imaging of posttrau-
85. Maravilla KR, Bowen BC. Imaging of the peripheral nervous matic brachial plexus injury. Clin Orthop 1988;237:57 61.
system: evaluation of peripheral neuropathy and plexopathy.
109. Roos DB. The thoracic outlet syndrome is underrated. Arch
AJNR 1998;19:10111023.
Neurol 1990;47:327328.
86. Mendelsohn RA, Weiner IH, Keegan JM. Myelographic dem-
110. Roos DB. Thoracic outlet syndrome is underdiagnosed. Mus-
onstration of brachial plexus root avulsion. Arch Surg 1957;
cle Nerve 1999;22:126 129.
75:102107.
111. Salner AL, Botnick LE, Herzog AG, Goldstein MA, Harris JR,
87. Meyer R. Treatment of obstetrical palsy. In: Omer GE Jr,
Levene MB, Hellman S. Reversible brachial plexopathy fol-
Spinner M, Van Beek AL, editors. Management of periph-
lowing primary radiation therapy for breast cancer. Cancer
eral nerve problems, 2nd ed. Philadelphia: WB Saunders;
Treat Rep 1981;65:797 802.
1998. p 454 458.
88. Miller DS, Boswick JA. Lesions of the brachial plexus associ- 112. Sanders EA, Van den Neste VM, Hoogenraad TU. Brachial
ated with fractures of the clavicle. Clin Orthop 1969;64:144 plexus neuritis and recurrent laryngeal nerve palsy. J Neurol
149. 1988;235:323.
89. Millesi H. Brachial plexus injury in adults: operative repair. 113. Seddon H. Surgical disorders of peripheral nerves. London:
In: Gelberman RH, editor. Operative nerve repair and re- Churchill Livingstone; 1975. 336 p.
construction, Vol 2. Philadelphia: Lippincott; 1991. p 1285 114. Seror P. Brachial plexus neoplastic lesions assessed by con-
1301. duction study of medial antebrachial cutaneous nerve. Mus-
90. Milton GW. The mechanism of circumex and other nerve cle Nerve 2001;24:1068 1070.
injuries in dislocation of the shoulder and the possible 115. Shoup D, Toffol GJ, Trahan TJ. Brachial plexopathy second-
mechanism of nerve injury during reduction of dislocation. ary to anticoagulant-induced hematoma as a complication of
Aust N Z J Surg 1953;23:2530. axillary arteriography. J Am Osteopath Assoc 1997;97:102
91. Mulvey DA, Aquilina RJ, Elliott MW, Moxham J, Green M. 105.
Diaphragmatic dysfunction in neuralgic amyotrophy: an 116. Sjoberg I, Erichs K, Bjerre I. Cause and effect of obstetric
electrophysiologic evaluation of 16 patients presenting with (neonatal) brachial plexus palsy. Acta Paediatr Scand 1988;
dyspnea. Am Rev Respir Dis 1993;147:66 71. 77:357364.
92. Mumenthaler M. Armplexusparesen im anschluss an ront- 117. Slingluff CL Jr, Terzis JK, Edgerton MT. The quantitative
genbestrahlung. Schweiz Med Wochenschr 1964;94:1069 microanatomy of the brachial plexus in man: reconstructive
1075. relevance. In: Terzis JK, editor. Microreconstruction of
93. Nagano A, Ochiai N, Sugioka H, Hara T, Tsuyama N. Use- nerve injuries. Philadelphia: WB Saunders; 1987. p 285324.
fulness of myelography in brachial plexus injuries. J Hand 118. Smith DC, Mitchell DA, Peterson GW, Will AD, Mera SS,
Surg 1989;14B:59 64. Smith LL. Medial brachial fascial compartment syndrome:
94. Narakas AO. The surgical treatment of traumatic brachial anatomic basis of neuropathy after transaxillary arteriogra-
plexus lesions. Int Surg 1980;6:521527. phy. Radiology 1989;173:149 154.
95. Narakas AO. Traumatic brachial plexus lesions. In: Dyck PJ, 119. Spinner RJ, Kline DG. Surgery for peripheral nerve and
Thomas PK, Lambert EH, Bunge R, editors. Peripheral neu- brachial plexus injuries or other nerve lesions. Muscle Nerve
ropathy, Vol 2. Philadelphia: WB Saunders; 1984. p 1393 2000;23:680 695.
1409. 120. Staal A, van Voorthuisen AE, van Dyck LM. Neurologic
96. Nishida T, Price SJ, Minieka MM. Medial antebrachial cutane- complication following arterial catheterization by the axil-
ous nerve conduction in true neurogenic thoracic outlet syn- lary approach. Br J Radiol 1966;39:115116.
drome. Electromyogr Clin Neurophysiol 1993;33:285288. 121. Stewart JD. Focal peripheral neuropathies, 2nd ed. New
97. OKeefe DM. Brachial plexus injury following axillary arte- York: Raven Press; 1993. 506 p.
riography: a case report and review of the literature. J Neu- 122. Stewart JD. Peripheral nerve fascicles: anatomy and clinical
rosurg 1980;53:853 857. relevance. Muscle Nerve 2003;28:525541.
Brachial Plexopathies MUSCLE & NERVE November 2004 567
123. Stoll BA, Andrews JT. Radiation-induced peripheral neurop- 142. Wilbourn AJ. Thoracic outlet syndrome surgery causing se-
athy. Br Med J 1966;1:834 837. vere brachial plexopathy. Muscle Nerve 1988;11:66 74.
124. Sunderland S. Meningeal-neural relations in the interverte- 143. Wilbourn AJ. The thoracic outlet syndrome is overdiag-
bral foramen. J Neurosurg 1974;40:756 763. nosed. Arch Neurol 1990;47:328 330.
125. Sunderland S. Nerves and nerve injuries, 2nd ed. London: 144. Wilbourn AJ. Brachial plexus disorders. In: Dyck PJ, Thomas
Churchill Livingstone; 1978. 1046 p. PK, editors. Peripheral neuropathy, 3rd ed. Philadelphia:
126. Thomas JE, Colby MY. Radiation-induced or metastatic bra- WB Saunders; 1993. p 911950.
chial plexopathy? A diagnostic dilemma. JAMA 1972;222: 145. Wilbourn AJ. Nerve injuries caused by injections and tour-
13921395. niquets. In: Syllabus on physical trauma to peripheral nerves
127. Thyagarajan D, Cascino T, Harms G. Magnetic resonance (1996 AAEM plenary session). Minneapolis: American Asso-
imaging in brachial plexopathy of cancer. Neurology 1995; ciation of Electrodiagnostic Medicine; 1996. p 1533.
45:421 427. 146. Wilbourn AJ. Iatrogenic nerve injuries. Neurol Clin 1998;16:
128. Toolanen G, Hildingsson C, Hedlund T, Knibestol M, Oberg 55 82.
L. Early complications after anterior dislocation of the shoul- 147. Wilbourn AJ. Thoracic outlet syndrome is overdiagnosed.
der in patients over 40 years: an ultrasonographic and elec- Muscle Nerve 1999;22:130 136.
tromyographic study. Acta Orthop Scand 1993;64:549 552. 148. Wilbourn AJ. Brachial plexopathies. In: Katirji B, Kaminski
129. Toshiyasu N, Yabe Y, Horiuchi Y, Takayama S. Magnetic HJ, Preston DC, Ruff RL, Shapiro BE, editors. Neuromuscu-
resonance myelography in brachial plexus injury. J Bone lar disorders in clinical practice. Boston: Butterworth Hei-
Joint Surg 1997;79B:764 769. nemann; 2002. p 884 906.
130. Trojaborg W. Clinical, electrophysiological, and myelo- 149. Wilbourn AJ, Aminoff MJ. Radiculopathies. In: Brown WF,
graphic studies of 9 patients with cervical spinal root avul- Bolton CF, editors. Clinical electromyography, 2nd ed. Bos-
sions: discrepancies between EMG and X-ray ndings. Mus- ton: Butterworth Heinemann; 1993. p 175205.
cle Nerve 1994;17:913922.
150. Wilbourn AJ, Ferrante MA. Plexopathies. In: Pourmand R,
131. Tsairis P, Dyck PJ, Mulder DW. Natural history of brachial
editor. Neuromuscular diseases: expert clinicians views. Bos-
plexus neuropathy: report on 99 patients. Arch Neurol 1972;
ton: Butterworth Heinemann; 2001. p 493527.
27:109 117.
132. Tsao BE, Wilbourn AJ. The medial brachial fascial compart- 151. Wilbourn AJ, Levin KH, Lederman RJ. Radiation-induced
ment syndrome following axillary arteriography. Neurology brachial plexopathy: electrodiagnostic changes over 13
2003;61:10371041. years. Muscle Nerve 1994;17:1108.
133. Ubachs JM, Slooff AC, Peeters LL. Obstetric antecedents of 152. Windebank AJ. Inherited recurrent focal neuropathies. In:
surgically treated obstetric brachial plexus injuries. Br J Ob- Dyck PJ, Thomas PK, Lambert EG, Bunge R, editors. Periph-
stet Gynaecol 1995;102:813 817. eral neuropathy, Vol 2. Philadelphia: Saunders; 1984. p
134. van Arfen N, van Engelen BG, Reinders JW, Kremer H, 1656 1670.
Gabreels FJ. The natural history of hereditary neuralgic 153. Wolf H, Hoeksma AF, Oei SL, Bleker OP. Obstetric brachial
amyotrophy on the Dutch population: two distinct types? plexus injury: risk factors related to recovery. Eur J Obstet
Brain 2000;123:718 723. Gynecol Reprod Biol 2000;88:133138.
135. Van Dijk JG, Pondaag W, Malessy MJA. Obstetric lesions of 154. Wolock B, Millesi H. Brachial plexus: applied anatomy and
the brachial plexus. Muscle Nerve 2001;24:14511461. operative exposure. In: Gelberman RH, editor. Operative
136. Vander Salm TJ, Cereda JM, Cutler BS. Brachial plexus nerve repair and reconstruction, Vol 2. Philadelphia: Lip-
injury following median sternotomy. J Thorac Cardiovasc pincott; 1991. p 12551272.
Surg 1980;80:447 452. 155. Wynn Parry CB. Brachial plexus injuries. In: Vinken PJ,
137. Vander Salm TJ, Cutler BS, Okike ON. Brachial plexus Bruyn GW, Klawans HL, editors. Handbook of clinical neu-
injury following median sternotomy. Part 2. J Thorac Car- rology, Vol 51. Amsterdam: Elsevier; 1987. p 143155.
diovasc Surg 1982;83:914 917. 156. Zimmerman NB, Weiland AJ. Assessment and monitoring of
138. Walsh JF. The anatomy of the brachial plexus. Am J Med Sci brachial plexus injury in the adult. In: Gelberman RH, edi-
1877;74:387398. tor. Operative nerve repair and reconstruction, Vol 2. Phil-
139. Watson BV, Nicolle MW, Brown JD. Conduction block in adelphia: Lippincott; 1991. p 12731283.
neuralgic amyotrophy. Muscle Nerve 2001;24:559 563. 157. Zipkin M, Backus WW, Scott B, Poppers PJ. False aneurysm
140. Watts GDJ, OBriant KC, Borreson TE, Windebank AJ, of the axillary artery following brachial plexus block. J Clin
Chance PF. Evidence for genetic heterogeneity in hereditary Anesth 1991;3:143145.
neuralgic amyotrophy. Neurology 2001;56:675 678. 158. Zorub D, Nashold B, Cook W. Avulsion of the brachial
141. Wilbourn AJ. Electrodiagnosis of plexopathies. Neurol Clin plexus I: a review with implications on the therapy of intrac-
1985;3:511529. table pain. Surg Neurol 1974;2:347353.
568 Brachial Plexopathies MUSCLE & NERVE November 2004
Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- INSERT All Values: Chapter 2: InsertingDokumen1 halamanINSERT All Values: Chapter 2: InsertingNishki GejmerBelum ada peringkat
- Second Normal Form: Chapter 1: CreatingDokumen1 halamanSecond Normal Form: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Fourth Normal Form: Chapter 1: CreatingDokumen1 halamanFourth Normal Form: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Fifth Normal Form: Chapter 1: CreatingDokumen1 halamanFifth Normal Form: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Boyce-Codd Normal Form: Chapter 1: CreatingDokumen1 halamanBoyce-Codd Normal Form: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Normalized Design: Chapter 1: CreatingDokumen1 halamanNormalized Design: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Third Normal Form: Chapter 1: CreatingDokumen1 halamanThird Normal Form: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter SummaryDokumen1 halamanChapter SummaryNishki GejmerBelum ada peringkat
- Inserting: N N N N NDokumen1 halamanInserting: N N N N NNishki GejmerBelum ada peringkat
- This Page Intentionally Left BlankDokumen1 halamanThis Page Intentionally Left BlankNishki GejmerBelum ada peringkat
- FOREIGN KEY Table Constraint: Chapter 1: CreatingDokumen1 halamanFOREIGN KEY Table Constraint: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- CREATE Remote and Proxy Tables: Chapter 1: CreatingDokumen1 halamanCREATE Remote and Proxy Tables: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: Creating: First Normal FormDokumen1 halamanChapter 1: Creating: First Normal FormNishki GejmerBelum ada peringkat
- Chapter 1: CreatingDokumen1 halamanChapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: CreatingDokumen1 halamanChapter 1: CreatingNishki GejmerBelum ada peringkat
- Temporary Tables: Chapter 1: CreatingDokumen1 halamanTemporary Tables: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Global Temporary Tables: Chapter 1: CreatingDokumen1 halamanGlobal Temporary Tables: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: CreatingDokumen1 halamanChapter 1: CreatingNishki GejmerBelum ada peringkat
- Free Space: Chapter 1: CreatingDokumen1 halamanFree Space: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- UNIQUE Table Constraint: Chapter 1: CreatingDokumen1 halamanUNIQUE Table Constraint: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Create Server: Chapter 1: CreatingDokumen1 halamanCreate Server: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Table CHECK Constraint: Chapter 1: CreatingDokumen1 halamanTable CHECK Constraint: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Foreign Key Column Constraint: Chapter 1: CreatingDokumen1 halamanForeign Key Column Constraint: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Free Space: Chapter 1: CreatingDokumen1 halamanFree Space: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: Creating: PRIMARY KEY Column ConstraintDokumen1 halamanChapter 1: Creating: PRIMARY KEY Column ConstraintNishki GejmerBelum ada peringkat
- User-Defined Data Types: UNIQUE Column ConstraintDokumen1 halamanUser-Defined Data Types: UNIQUE Column ConstraintNishki GejmerBelum ada peringkat
- Special Update Defaults: Chapter 1: CreatingDokumen1 halamanSpecial Update Defaults: Chapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: CreatingDokumen1 halamanChapter 1: CreatingNishki GejmerBelum ada peringkat
- Chapter 1: Creating: NOT NULL ConstraintDokumen1 halamanChapter 1: Creating: NOT NULL ConstraintNishki GejmerBelum ada peringkat
- Expressions As Defaults: NULL PropertyDokumen1 halamanExpressions As Defaults: NULL PropertyNishki GejmerBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 2 National Admission and Discharge Protocols For Ethiopian Hospitals November, 2012Dokumen76 halaman2 National Admission and Discharge Protocols For Ethiopian Hospitals November, 2012Siham Si Seid67% (3)
- VP Sales Medical Devices in Dallas FT Worth TX Resume John GilbertDokumen3 halamanVP Sales Medical Devices in Dallas FT Worth TX Resume John GilbertJohnGilbertBelum ada peringkat
- SIP Poster - Hannah PR2Dokumen1 halamanSIP Poster - Hannah PR2NCPQSWBelum ada peringkat
- Initial Nurse - Docx NPI NPIDokumen22 halamanInitial Nurse - Docx NPI NPIIyanna BaylonBelum ada peringkat
- Acute Vertigo in A Man of 52Dokumen3 halamanAcute Vertigo in A Man of 52Mahmood MuftiBelum ada peringkat
- Children Do Well If They CanDokumen57 halamanChildren Do Well If They CanatmarshBelum ada peringkat
- Medical Negligence ProjectDokumen40 halamanMedical Negligence ProjectIshank Singh100% (1)
- Skilled Discharge Planning FormDokumen3 halamanSkilled Discharge Planning FormRini Fauzia ABelum ada peringkat
- Burns PresentationDokumen84 halamanBurns PresentationMaria BudnicBelum ada peringkat
- Hospital Accreditation QuestionsDokumen5 halamanHospital Accreditation Questionsshoumyaosu100% (21)
- 2014-010632 MX RPT FinalDokumen10 halaman2014-010632 MX RPT FinalHariadi WidodoBelum ada peringkat
- Community Helpers RhymesDokumen10 halamanCommunity Helpers RhymesAarti NaiduBelum ada peringkat
- Concept Art TheoryDokumen11 halamanConcept Art Theoryapi-278085794Belum ada peringkat
- Job Satisfaction of Rural Nurses in District Hospitals in The Province of LeyteDokumen64 halamanJob Satisfaction of Rural Nurses in District Hospitals in The Province of LeyteJoanneRoseKintana100% (10)
- Founder Fellows: Tamilnadu Academy of Sciences, Chennai, 1976Dokumen5 halamanFounder Fellows: Tamilnadu Academy of Sciences, Chennai, 1976Ponnusamy RamalingamBelum ada peringkat
- The Silent Death of Americas ChildrenDokumen15 halamanThe Silent Death of Americas ChildrenIlaMarie73Belum ada peringkat
- Institutional Minimum Req Off-Street DavidDokumen2 halamanInstitutional Minimum Req Off-Street DavidMikealla DavidBelum ada peringkat
- Jurisprudence and Legal Liabilities in NursingDokumen32 halamanJurisprudence and Legal Liabilities in Nursingzade89080% (5)
- Business PlanDokumen5 halamanBusiness Planapi-292411774Belum ada peringkat
- Narayana Hrudayalaya - Section C - Group 5Dokumen22 halamanNarayana Hrudayalaya - Section C - Group 5raushanrahulBelum ada peringkat
- Chamberlain College of Nursing: Name: DateDokumen6 halamanChamberlain College of Nursing: Name: DategabrielBelum ada peringkat
- Stretch & SweepDokumen3 halamanStretch & SweepYwagar YwagarBelum ada peringkat
- Bone Lengthening Procedure (Ilizarov Method) : Seminar, Workshop & Live SurgeryDokumen4 halamanBone Lengthening Procedure (Ilizarov Method) : Seminar, Workshop & Live SurgerypradhanaadhityaBelum ada peringkat
- A Call For The Development of Advanced Practice Nursing in The PhilippinesDokumen11 halamanA Call For The Development of Advanced Practice Nursing in The Philippinesjaspertolarba100% (3)
- Plac Pathology - Drucilla RobertsDokumen11 halamanPlac Pathology - Drucilla RobertsconstantinilieBelum ada peringkat
- Uphs GuideDokumen2 halamanUphs GuideCristan Dave ZablanBelum ada peringkat
- AMC Building Regulations 2012Dokumen80 halamanAMC Building Regulations 2012oscar angelBelum ada peringkat
- 2 Clinical Need and Practice: Trauma-Ta74/the-TechnologyDokumen16 halaman2 Clinical Need and Practice: Trauma-Ta74/the-TechnologyherlilieBelum ada peringkat
- Ict 101 Project Ay 2012-201sampleDokumen9 halamanIct 101 Project Ay 2012-201sampleImusic KurokoBelum ada peringkat
- Mahnaz Shoghi Mahnaz Sanjari Workplace Violence and Abuse Against Nurses IDokumen10 halamanMahnaz Shoghi Mahnaz Sanjari Workplace Violence and Abuse Against Nurses IHamidreza MotalebiBelum ada peringkat