Anda mungkin juga menyukai
- Funny StoriesDokumen5 halamanFunny Storiesamin jamalBelum ada peringkat
- Medicaid Provider Enrollment Guide 2011Dokumen18 halamanMedicaid Provider Enrollment Guide 2011Patrick PerezBelum ada peringkat
- Denial Action Training: Welcome To AllDokumen25 halamanDenial Action Training: Welcome To Allbraney miller100% (6)
- The Effectiveness of Psychodynamic Psychotherapies - An Update (2015) PDFDokumen14 halamanThe Effectiveness of Psychodynamic Psychotherapies - An Update (2015) PDFmysticmdBelum ada peringkat
- Making Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchDokumen36 halamanMaking Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchNational Pharmaceutical CouncilBelum ada peringkat
- PhilamCare Health Systems Ruling on Insurance Contract RescissionDokumen2 halamanPhilamCare Health Systems Ruling on Insurance Contract RescissionkamiruhyunBelum ada peringkat
- Professional Communication in NursingDokumen100 halamanProfessional Communication in NursingPearl DiBerardino100% (2)
- Using Pragmatic Clinical Trials To Test The Effectiveness of Patient-Centered Medical Home Models in Real-World Settings PCMH Research Methods SeriesDokumen11 halamanUsing Pragmatic Clinical Trials To Test The Effectiveness of Patient-Centered Medical Home Models in Real-World Settings PCMH Research Methods SeriesJames LindonBelum ada peringkat
- 未知Dokumen6 halaman未知Haiying MaoBelum ada peringkat
- Unraveling The Potential of Real-World Studies (2017)Dokumen4 halamanUnraveling The Potential of Real-World Studies (2017)Arturo Lopez GilBelum ada peringkat
- Setting A Research Agenda For Medical Over UseDokumen7 halamanSetting A Research Agenda For Medical Over UsemmBelum ada peringkat
- Economic Evaluation in Critical CareDokumen10 halamanEconomic Evaluation in Critical Careapi-3832022Belum ada peringkat
- tmp4F9 TMPDokumen7 halamantmp4F9 TMPFrontiersBelum ada peringkat
- Clinical TrialDokumen2 halamanClinical TrialRajesh GyawaliBelum ada peringkat
- Practical Clinical Trials: Increasing The Value of Clinical Research For Decision Making in Clinical and Health PolicyDokumen9 halamanPractical Clinical Trials: Increasing The Value of Clinical Research For Decision Making in Clinical and Health PolicyJim MorrisonBelum ada peringkat
- Mr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaDokumen6 halamanMr. Hariom Rajput Mr. Ramsingh Ji Gmail-ID International Association of Oncology (IAO) Government of IndiaHariom RajputBelum ada peringkat
- Moving Beyond RCTs for Public Health EvidenceDokumen6 halamanMoving Beyond RCTs for Public Health EvidenceSamuel Andrés AriasBelum ada peringkat
- Lorne Basskin - Practical PE ArticleDokumen5 halamanLorne Basskin - Practical PE ArticleCatalina Dumitru0% (1)
- MODELDokumen41 halamanMODELGenesis BiceraBelum ada peringkat
- Multi-Criteria Clinical Decision Support - A Primer On The Use of Multiple Criteria Decision Making Methods To Promote Evidence-Based, Patient-Centered HealthcareDokumen17 halamanMulti-Criteria Clinical Decision Support - A Primer On The Use of Multiple Criteria Decision Making Methods To Promote Evidence-Based, Patient-Centered HealthcareabebotalardyBelum ada peringkat
- Gesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Dokumen15 halamanGesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Stavros TheodoridisBelum ada peringkat
- Using Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common PitfallsDokumen7 halamanUsing Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common Pitfallsujangketul62Belum ada peringkat
- Assessing The Value of Healthcare Interventions Using Multi-Criteria Decision Analysis: A Review of The LiteratureDokumen21 halamanAssessing The Value of Healthcare Interventions Using Multi-Criteria Decision Analysis: A Review of The LiteratureLiz BLBelum ada peringkat
- Evidence Based Medication General Guidelines For Clinical Pharmacy PracticeDokumen10 halamanEvidence Based Medication General Guidelines For Clinical Pharmacy PracticeMahum SohailBelum ada peringkat
- Chapter 12 Systematic Review of Prognostic TestsDokumen13 halamanChapter 12 Systematic Review of Prognostic TestsMuammar EmirBelum ada peringkat
- World Psychiatry - 2015 - Fonagy - The Effectiveness of Psychodynamic Psychotherapies An UpdateDokumen14 halamanWorld Psychiatry - 2015 - Fonagy - The Effectiveness of Psychodynamic Psychotherapies An UpdateJunior BonfáBelum ada peringkat
- 1 Health Econ Rodriguez 2013Dokumen7 halaman1 Health Econ Rodriguez 2013EgociBelum ada peringkat
- Creating win-win relationships through contestabilityDokumen2 halamanCreating win-win relationships through contestabilitymchelemBelum ada peringkat
- JDS 712Dokumen9 halamanJDS 712aaditya01Belum ada peringkat
- A Randomized Controlled Trial of A Computer-Based Physician Workstation in An Outpatient Setting: Implementation Barriers To Outcome EvaluationDokumen9 halamanA Randomized Controlled Trial of A Computer-Based Physician Workstation in An Outpatient Setting: Implementation Barriers To Outcome EvaluationDith Rivelta CallahanthBelum ada peringkat
- 1986 - A Framework For Clinical Evaluation of Diagnostic TechnologiesDokumen8 halaman1986 - A Framework For Clinical Evaluation of Diagnostic TechnologiesA CBelum ada peringkat
- Decision Support System Literature ReviewDokumen6 halamanDecision Support System Literature Reviewc5j2ksrg100% (1)
- Delivering Outstanding Medical Care Requires Evidence-Based Decision SupportDokumen8 halamanDelivering Outstanding Medical Care Requires Evidence-Based Decision SupportTTJBelum ada peringkat
- Nejm CER Consent KassDokumen3 halamanNejm CER Consent KassSasha Hidayat FullBelum ada peringkat
- Jamainternal Anderson 2020 Ic 200009Dokumen2 halamanJamainternal Anderson 2020 Ic 200009cornelia sianturiBelum ada peringkat
- 11.1 Diagnostic Tests 1-S2.0-S0001299818300941-MainDokumen7 halaman11.1 Diagnostic Tests 1-S2.0-S0001299818300941-MainHelioPassulequeBelum ada peringkat
- Running Head: Health Informatics 1Dokumen6 halamanRunning Head: Health Informatics 1Vishal VijBelum ada peringkat
- Meta Analysis Nursing Literature ReviewDokumen10 halamanMeta Analysis Nursing Literature Reviewea46krj6100% (1)
- The US Payor Landscape: Results From A Survey of Medical Directors and Pharmacy Directors On Comparative-Effectiveness ResearchDokumen7 halamanThe US Payor Landscape: Results From A Survey of Medical Directors and Pharmacy Directors On Comparative-Effectiveness ResearchSabrina JonesBelum ada peringkat
- Evidence-Based Clinical Decision Support (CDS) : Terry Seaton, Pharm.D., FCCP, BCPS Professor of Pharmacy PracticeDokumen26 halamanEvidence-Based Clinical Decision Support (CDS) : Terry Seaton, Pharm.D., FCCP, BCPS Professor of Pharmacy PracticeTroyBelum ada peringkat
- Pharmacoeconomics: Basic Concepts and Terminology: T. Walley & A. HaycoxDokumen6 halamanPharmacoeconomics: Basic Concepts and Terminology: T. Walley & A. HaycoxIndra PratamaBelum ada peringkat
- Beyond The Headlines: Unveiling The Power of Clinical TrialsDokumen4 halamanBeyond The Headlines: Unveiling The Power of Clinical Trialsamazingworldview7Belum ada peringkat
- Early drug discovery and development guidelinesDokumen43 halamanEarly drug discovery and development guidelinesprashantBelum ada peringkat
- 2022 V13i12025Dokumen5 halaman2022 V13i12025kmp pssrBelum ada peringkat
- Literature Review On Medication Errors in HospitalsDokumen7 halamanLiterature Review On Medication Errors in Hospitalsfvgjcq6aBelum ada peringkat
- Rational Decision Making in MedicineDokumen11 halamanRational Decision Making in MedicineSanti AraratBelum ada peringkat
- Metanalisis Adherencia Al TratamientoDokumen9 halamanMetanalisis Adherencia Al TratamientosergioBelum ada peringkat
- The Impact of Health Information Technology On Patient SafetyDokumen13 halamanThe Impact of Health Information Technology On Patient SafetySaba Abu FarhaBelum ada peringkat
- Dissertation Randomised Controlled TrialDokumen4 halamanDissertation Randomised Controlled TrialBuyAPaperOnlineUK100% (1)
- Advancing Drug Safety PDFDokumen3 halamanAdvancing Drug Safety PDFjohnBelum ada peringkat
- Basic PDFDokumen2 halamanBasic PDFAshilla ShafaBelum ada peringkat
- Clinical Decision Support SystemDokumen8 halamanClinical Decision Support SystemJieshun WangBelum ada peringkat
- Stat & ResearchDokumen276 halamanStat & ResearchSYED ALI HUSSAINBelum ada peringkat
- Reversals of Established Medical Practices: Evidence To Abandon ShipDokumen4 halamanReversals of Established Medical Practices: Evidence To Abandon ShipuoleoauBelum ada peringkat
- Qaly 2 PDFDokumen4 halamanQaly 2 PDFApril ayuBelum ada peringkat
- Wiley Milbank Memorial FundDokumen42 halamanWiley Milbank Memorial FundLuciana NovaesBelum ada peringkat
- The Science of Clinical Practice - Disease Diagnosis or Patient Prognosis - Croft Et Al 2015Dokumen8 halamanThe Science of Clinical Practice - Disease Diagnosis or Patient Prognosis - Croft Et Al 2015Bipul RajbhandariBelum ada peringkat
- Mental Health Services Research Methodology 2002Dokumen8 halamanMental Health Services Research Methodology 2002Kats CoelloBelum ada peringkat
- Baccountingackground Researc1Dokumen6 halamanBaccountingackground Researc1Noor Ul AinBelum ada peringkat
- Real-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsDokumen5 halamanReal-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsCognizantBelum ada peringkat
- 2022 V13i12025Dokumen5 halaman2022 V13i12025kmp pssrBelum ada peringkat
- Murphy 2021Dokumen11 halamanMurphy 2021okBelum ada peringkat
- Developing Treatment Guidelines For Myasthenia GravisDokumen7 halamanDeveloping Treatment Guidelines For Myasthenia GravismoneurBelum ada peringkat
- Perspective: New England Journal MedicineDokumen4 halamanPerspective: New England Journal MedicineYRHLI7389Belum ada peringkat
- Clinical Decision Support System: Fundamentals and ApplicationsDari EverandClinical Decision Support System: Fundamentals and ApplicationsBelum ada peringkat
- Wound 2016 0720Dokumen10 halamanWound 2016 0720Lucky Permana100% (1)
- James Square LawsuitDokumen28 halamanJames Square LawsuitAnonymous 3xG5yujMVc100% (1)
- 55 Plus: A Manitoba Income SupplementDokumen1 halaman55 Plus: A Manitoba Income SupplementDJ MedinaBelum ada peringkat
- Tricare Report Dec. 2007Dokumen204 halamanTricare Report Dec. 2007GovtfraudlawyerBelum ada peringkat
- Welcome Guide Seidman Cancer CenterDokumen26 halamanWelcome Guide Seidman Cancer CenterAnonymous zHDhriXBelum ada peringkat
- Hold Harmless AgreementDokumen2 halamanHold Harmless Agreementapi-282593087Belum ada peringkat
- Excellence in Patient Satisfaction Within A Patient-Centered CultureDokumen4 halamanExcellence in Patient Satisfaction Within A Patient-Centered CultureYepi AboucathBelum ada peringkat
- Go 174Dokumen5 halamanGo 174api-218060126Belum ada peringkat
- C Ovid 19 Positive Test Report FormDokumen2 halamanC Ovid 19 Positive Test Report FormMinaketan DasBelum ada peringkat
- Advantages and Disadvantages of Free Health CareDokumen4 halamanAdvantages and Disadvantages of Free Health CareSam kBelum ada peringkat
- Individual Short FormDokumen5 halamanIndividual Short FormJenifer SanchezBelum ada peringkat
- 2017 T1DF Test Strips Action - Complaint (Case 2:17-cv-00803 Filed by Keller Rohrback On May 24, 2017)Dokumen274 halaman2017 T1DF Test Strips Action - Complaint (Case 2:17-cv-00803 Filed by Keller Rohrback On May 24, 2017)The Type 1 Diabetes Defense FoundationBelum ada peringkat
- Annual Report 2011Dokumen28 halamanAnnual Report 2011vnatcBelum ada peringkat
- Chapter 5 Demand For Medical Services4784Dokumen52 halamanChapter 5 Demand For Medical Services4784RI NABelum ada peringkat
- Mental Health Services Directory November 2014Dokumen83 halamanMental Health Services Directory November 2014api-279173964Belum ada peringkat
- 2018 Medicare Physician Fee Schedule SLPDokumen14 halaman2018 Medicare Physician Fee Schedule SLPAnonymous WpMUZCb935Belum ada peringkat
- Physician Authorization Form For Custom Panels (Single Physician)Dokumen2 halamanPhysician Authorization Form For Custom Panels (Single Physician)Anonymous AJEXGWzOBelum ada peringkat
- Test Bank For Medical Insurance 8th Edition by ValeriusDokumen16 halamanTest Bank For Medical Insurance 8th Edition by ValeriusroytuyenbauBelum ada peringkat
- Healthcare Insurance Company Case Study - 3Dokumen1 halamanHealthcare Insurance Company Case Study - 3api-482448129Belum ada peringkat
- 2nd Sem NCPDokumen1 halaman2nd Sem NCPFryd Ryxx GarciaBelum ada peringkat
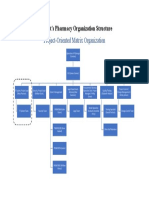
- Wilmont Organization Structure-Wilmont's PharmacyDokumen1 halamanWilmont Organization Structure-Wilmont's PharmacySalah Ud DinBelum ada peringkat
- Shouldice PDFDokumen2 halamanShouldice PDFRizvi SyedBelum ada peringkat
- AHCM HealthSocialNeedsScreeningTool Rev 8 - 10 - 2021Dokumen10 halamanAHCM HealthSocialNeedsScreeningTool Rev 8 - 10 - 2021submarinoaguadulceBelum ada peringkat
- Health Advocate's StoryDokumen4 halamanHealth Advocate's StoryHealth Advocate, Inc.Belum ada peringkat
- State of Minnesota's EMSDokumen2 halamanState of Minnesota's EMSMichael JohnsonBelum ada peringkat