Anda mungkin juga menyukai
- Cystitis, A Simple Guide To The Condition Treatment And Urinary DiseasesDari EverandCystitis, A Simple Guide To The Condition Treatment And Urinary DiseasesBelum ada peringkat
- The Effect of Urinary Tract Infections in Elderly People With and Without DiabetesDokumen5 halamanThe Effect of Urinary Tract Infections in Elderly People With and Without DiabetesInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Uti ReadingsDokumen6 halamanUti ReadingskarenbelnasBelum ada peringkat
- Simple Laboratory Test For Urine-FinalDokumen77 halamanSimple Laboratory Test For Urine-FinalPaul John ToralBelum ada peringkat
- Theoretical Background Urinary Tract InfectionDokumen7 halamanTheoretical Background Urinary Tract Infectiondenebrench23Belum ada peringkat
- DiabetesDokumen1 halamanDiabetesJobelle Rodriguez BernabeBelum ada peringkat
- Prevalence of Uti in Benin PDFDokumen54 halamanPrevalence of Uti in Benin PDFcamiladovalle95Belum ada peringkat
- Acute Simple Cystitis in Women - UpToDateDokumen29 halamanAcute Simple Cystitis in Women - UpToDateMédico NautaBelum ada peringkat
- Name: Bernasha Septianita NIM: 151810113037Dokumen2 halamanName: Bernasha Septianita NIM: 151810113037NachayaBelum ada peringkat
- Uti Case StudyDokumen7 halamanUti Case StudyStephBelum ada peringkat
- Prevalence of Uti in BeninDokumen49 halamanPrevalence of Uti in Benincamiladovalle95Belum ada peringkat
- Dysuria in AdultsDokumen8 halamanDysuria in AdultsSi vis pacem...Belum ada peringkat
- An Individual Case Study Entitled PYELONEPHRITISDokumen12 halamanAn Individual Case Study Entitled PYELONEPHRITISShane JacobBelum ada peringkat
- Urinary Tract Infections in Pregnancy: BackgroundDokumen18 halamanUrinary Tract Infections in Pregnancy: BackgroundAqeel AhmedBelum ada peringkat
- Infeksi Saluran KemihDokumen65 halamanInfeksi Saluran KemihHaziq AnuarBelum ada peringkat
- Family Medicine COPCDokumen20 halamanFamily Medicine COPCrachellesliedeleonBelum ada peringkat
- Readings: Acute PyelonephritisDokumen6 halamanReadings: Acute PyelonephritisMauriceBelum ada peringkat
- UTIDokumen6 halamanUTIAyessa Marie BarbosaBelum ada peringkat
- Laboratory Work in Bio 102: Microbiology and Parasitology Laboratory Activity No. 5Dokumen2 halamanLaboratory Work in Bio 102: Microbiology and Parasitology Laboratory Activity No. 5DELOS SANTOS JESSIECAHBelum ada peringkat
- Public Health Aspects of Urogenital System Diseases: Irwin Aras/ Andi Alfian ZainuddinDokumen40 halamanPublic Health Aspects of Urogenital System Diseases: Irwin Aras/ Andi Alfian ZainuddinSadam_fasterBelum ada peringkat
- Urinary Tract Infection: Causes, Symptoms, Diagnosis and It's ManagementDokumen8 halamanUrinary Tract Infection: Causes, Symptoms, Diagnosis and It's ManagementAyat RajpootBelum ada peringkat
- Urinary Tract Infection in AdultsDokumen8 halamanUrinary Tract Infection in AdultsFeenyxBelum ada peringkat
- Uti PathoDokumen15 halamanUti PathoEden Astred ObilloBelum ada peringkat
- By: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzaDokumen19 halamanBy: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzajbaawuoBelum ada peringkat
- Case-Study-Journal LololDokumen25 halamanCase-Study-Journal LololDeannBelum ada peringkat
- Urinary Tract Infections د.أحمد الأهنوميDokumen44 halamanUrinary Tract Infections د.أحمد الأهنوميMohammad BelbahaithBelum ada peringkat
- (H.T.T.T.C) : Choose Any Physiology Taught and Do A Power Point Lay Out Physiology: Urinary SystemDokumen11 halaman(H.T.T.T.C) : Choose Any Physiology Taught and Do A Power Point Lay Out Physiology: Urinary SystemMunyen Renee-zitaBelum ada peringkat
- Clinical Presentations and Epidemiology of Urinary Tract InfectionsDokumen11 halamanClinical Presentations and Epidemiology of Urinary Tract InfectionsdimasBelum ada peringkat
- Background: Urinary Tract InfectionDokumen9 halamanBackground: Urinary Tract InfectionOnieBoy CurayagBelum ada peringkat
- UTI (Urinary Tract Infection)Dokumen9 halamanUTI (Urinary Tract Infection)Carson BirthBelum ada peringkat
- The Urinary System. The Urinary System Helps Maintain Proper Water and Salt Balance ThroughoutDokumen4 halamanThe Urinary System. The Urinary System Helps Maintain Proper Water and Salt Balance ThroughoutArjay EspañolBelum ada peringkat
- Cystitis in FemalesDokumen2 halamanCystitis in FemalesPatricia YohanaBelum ada peringkat
- Function of The Urinary SystemDokumen2 halamanFunction of The Urinary SystemniknokaBelum ada peringkat
- Written Assignment 7 Hs2211Dokumen7 halamanWritten Assignment 7 Hs2211Cali GureBelum ada peringkat
- Acute Simple Cystitis in Females - UpToDateDokumen29 halamanAcute Simple Cystitis in Females - UpToDateLaís FialhoBelum ada peringkat
- Case Study 8 (Urinary) - PyelonephritisDokumen7 halamanCase Study 8 (Urinary) - PyelonephritisSamantha AquinoBelum ada peringkat
- Biology Project 2018-19 Holiday HomeworkDokumen7 halamanBiology Project 2018-19 Holiday HomeworkMayukhi PaulBelum ada peringkat
- Urinary Tract Infection UTI and Dementia FactsheetDokumen10 halamanUrinary Tract Infection UTI and Dementia FactsheettoobaziBelum ada peringkat
- PPT-Acute PyeloDokumen117 halamanPPT-Acute PyeloJudy UrciaBelum ada peringkat
- UTI in AdultsDokumen4 halamanUTI in Adultsjoan_padilla2000Belum ada peringkat
- Urinary Tract Infection and QuinolonesDokumen49 halamanUrinary Tract Infection and QuinolonesKhanzada ShahzebBelum ada peringkat
- Urinary Tract Infections, Pyelonephritis, and ProstatitisDokumen27 halamanUrinary Tract Infections, Pyelonephritis, and Prostatitisnathan asfahaBelum ada peringkat
- Matas 2020Dokumen9 halamanMatas 2020Aubrey PerezBelum ada peringkat
- Renal InfectionDokumen5 halamanRenal InfectionNaqash NobleBelum ada peringkat
- Iaat 12 I 9 P 187Dokumen8 halamanIaat 12 I 9 P 187Maniak LuckBelum ada peringkat
- Itu EmgDokumen26 halamanItu EmgPaola Reyna O.Belum ada peringkat
- Chapter One 1.1 Background of StudyDokumen34 halamanChapter One 1.1 Background of Studyyusufgarba2002Belum ada peringkat
- Urinary Tract Infections - UpToDate-2022Dokumen30 halamanUrinary Tract Infections - UpToDate-2022Anna De AguasBelum ada peringkat
- Case Study (Uti)Dokumen6 halamanCase Study (Uti)Bible EvergardenBelum ada peringkat
- Urinary Tract InfectionsDokumen17 halamanUrinary Tract Infectionss.khan9211rediffmail.comBelum ada peringkat
- Symptoms: For Bladder InfectionsDokumen5 halamanSymptoms: For Bladder InfectionsGene Ryuzaki SeseBelum ada peringkat
- Infection Urinary Tract Urine Bladder KidneyDokumen18 halamanInfection Urinary Tract Urine Bladder KidneygdquijanoBelum ada peringkat
- Seminar On: Urinary Tract Infections and NephritisDokumen34 halamanSeminar On: Urinary Tract Infections and NephritisGargi MPBelum ada peringkat
- EtiologyDokumen15 halamanEtiologyrendyjiwonoBelum ada peringkat
- Types of Urinary Tract InfectionDokumen4 halamanTypes of Urinary Tract InfectionGencris Medrano Giray RNBelum ada peringkat
- UTI in DM - Super PaperDokumen6 halamanUTI in DM - Super PaperLourdes Fernandez CabreraBelum ada peringkat
- Urinary Complaints: Aviva Romm, Eric L. Yarnell, David WinstonDokumen16 halamanUrinary Complaints: Aviva Romm, Eric L. Yarnell, David WinstonIoana Mădălina BrînzăBelum ada peringkat
- Basilio Aya Nov 12 2016: ReadingDokumen5 halamanBasilio Aya Nov 12 2016: ReadingAyaBasilioBelum ada peringkat
- ProjDokumen12 halamanProjرافعہ میر بٹBelum ada peringkat
- Plenary Discussion Blok 21 Rio CoverDokumen1 halamanPlenary Discussion Blok 21 Rio CoverRijal Maulana HaqimBelum ada peringkat
- Rijal Maulana HaqimDokumen8 halamanRijal Maulana HaqimRijal Maulana HaqimBelum ada peringkat
- Unit 1 Language and Culture: Task 1 (Warm Up)Dokumen7 halamanUnit 1 Language and Culture: Task 1 (Warm Up)Rijal Maulana HaqimBelum ada peringkat
- Jadwal Jaga Puskesmas Imogiri 1 Koas ObsgynDokumen1 halamanJadwal Jaga Puskesmas Imogiri 1 Koas ObsgynRijal Maulana HaqimBelum ada peringkat
- Form Misc Blok 22Dokumen2 halamanForm Misc Blok 22Rijal Maulana HaqimBelum ada peringkat
- BLOK 22 - Community Medicine: Form MISC Form MISC Hippocampus 2012Dokumen2 halamanBLOK 22 - Community Medicine: Form MISC Form MISC Hippocampus 2012Rijal Maulana HaqimBelum ada peringkat
- Jadwal Jaga Puskesmas Imogiri 1 Koas ObsgynDokumen1 halamanJadwal Jaga Puskesmas Imogiri 1 Koas ObsgynRijal Maulana HaqimBelum ada peringkat
- Salivary MucocelesDokumen3 halamanSalivary MucocelesnsatriotomoBelum ada peringkat
- Infección Urinaria en Niños - NICEDokumen31 halamanInfección Urinaria en Niños - NICESu Paola Sanchez DávilaBelum ada peringkat
- Ayurvedic Treatment, Jiva Ayurveda MedicinesDokumen12 halamanAyurvedic Treatment, Jiva Ayurveda MedicinesAlbar MattaBelum ada peringkat
- UrinalysisDokumen2 halamanUrinalysisKiersten Karen Policarpio VerinaBelum ada peringkat
- HematuriaDokumen7 halamanHematuriaAgi TaronBelum ada peringkat
- Hardy CHROMUTIDokumen8 halamanHardy CHROMUTIJhonatan CastilloBelum ada peringkat
- Urology Questions Bank PDFDokumen16 halamanUrology Questions Bank PDFPalwasha Malik40% (5)
- Poltekkes URINARIA 2016Dokumen116 halamanPoltekkes URINARIA 2016Ayu Romadhona WinataBelum ada peringkat
- Root Cause AnalysisDokumen1 halamanRoot Cause AnalysisTri Hastuti HendrayaniBelum ada peringkat
- Thesis Topics Gynaecology ObstetricsDokumen7 halamanThesis Topics Gynaecology Obstetricsoaehviiig100% (2)
- Name: - Roll No. - Date: - Total Marks:65Dokumen8 halamanName: - Roll No. - Date: - Total Marks:65You TuberBelum ada peringkat
- Abdominal Pain During PregnancyDokumen64 halamanAbdominal Pain During Pregnancykhadzx100% (2)
- Urinary Germicides PharmaDokumen11 halamanUrinary Germicides PharmaMaria Pina Barbado PonceBelum ada peringkat
- Chapter 139: Urinary Tract Infections Self-Assessment QuestionsDokumen4 halamanChapter 139: Urinary Tract Infections Self-Assessment QuestionsTop VidsBelum ada peringkat
- RS CoachingDokumen201 halamanRS CoachingHalia MalicBelum ada peringkat
- Uti CPG 2Dokumen36 halamanUti CPG 2Yohan VeissmanBelum ada peringkat
- Strategic Intervention Materials PresentationDokumen55 halamanStrategic Intervention Materials PresentationMary Athena Ibardaloza Adesna100% (15)
- Perbandingan Leukosituria, Nitrit, Leukosit Esterase Dengan Kultur Urin Dalam Mendiagnosis Infeksi Saluran Kemih Pada AnakDokumen10 halamanPerbandingan Leukosituria, Nitrit, Leukosit Esterase Dengan Kultur Urin Dalam Mendiagnosis Infeksi Saluran Kemih Pada AnakFootball SonBelum ada peringkat
- Ure Thro CeleDokumen3 halamanUre Thro CeleKusum RoyBelum ada peringkat
- Antenatal Complications Acute ChronicDokumen10 halamanAntenatal Complications Acute ChronicJennie KimBelum ada peringkat
- Review of Functional Health Patterns (Gordon'S) : Block C - Group 2Dokumen9 halamanReview of Functional Health Patterns (Gordon'S) : Block C - Group 2Jam Dio Jubille PamogasBelum ada peringkat
- Urinary System WorksheetDokumen4 halamanUrinary System WorksheetTENNESSEE AYALABelum ada peringkat
- 104 Bactiguard BulletinDokumen12 halaman104 Bactiguard BulletinISCRRBelum ada peringkat
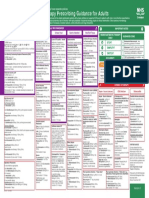
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDokumen1 halamanEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayBelum ada peringkat
- Medical-Surgical Nursing QuizDokumen3 halamanMedical-Surgical Nursing QuizGerald Resubal Oriña100% (1)
- Bladder IrrigationDokumen6 halamanBladder IrrigationKent Martin AmorosoBelum ada peringkat
- Prometric High-Yield NOTES PDFDokumen135 halamanPrometric High-Yield NOTES PDFDr-Jahanzaib Gondal100% (3)
- Evaluation of Abdominal PainDokumen7 halamanEvaluation of Abdominal PainCherry Faith Merisco LabtangBelum ada peringkat
- Urinary Tract Infection PIAG 84Dokumen3 halamanUrinary Tract Infection PIAG 84madimadi11Belum ada peringkat
- 1 Urology Care FoundationDokumen24 halaman1 Urology Care FoundationIntan Nur PratiwiBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (29)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Dari EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Penilaian: 3 dari 5 bintang3/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (81)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDari EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (328)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceDari EverandTo Explain the World: The Discovery of Modern SciencePenilaian: 3.5 dari 5 bintang3.5/5 (51)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 4 dari 5 bintang4/5 (5)
- Troubled: A Memoir of Foster Care, Family, and Social ClassDari EverandTroubled: A Memoir of Foster Care, Family, and Social ClassPenilaian: 4.5 dari 5 bintang4.5/5 (27)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDari EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifePenilaian: 4.5 dari 5 bintang4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDari EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 4 dari 5 bintang4/5 (4)
- The Marshmallow Test: Mastering Self-ControlDari EverandThe Marshmallow Test: Mastering Self-ControlPenilaian: 4.5 dari 5 bintang4.5/5 (59)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDari EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryPenilaian: 4 dari 5 bintang4/5 (45)