Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- (1292010120529 PM) B - Maternity Enrolment Form - EnglishDokumen2 halaman(1292010120529 PM) B - Maternity Enrolment Form - EnglishManzini Mlebogeng50% (2)
- 2015 Step2CK SampleItemsDokumen40 halaman2015 Step2CK SampleItemspreethamBelum ada peringkat
- Treatment of Lyme Disease - UpToDateDokumen4 halamanTreatment of Lyme Disease - UpToDateRoxana StanciuBelum ada peringkat
- HPV Lay LectureDokumen32 halamanHPV Lay LectureGene LynBelum ada peringkat
- Chronic CholecystitisDokumen6 halamanChronic CholecystitisIbraheem SairiBelum ada peringkat
- Maret 2021Dokumen36 halamanMaret 2021Muhammad Pahlan PiruzziBelum ada peringkat
- Enfermedad Renal CrónicaDokumen41 halamanEnfermedad Renal CrónicaAndrea MedinaBelum ada peringkat
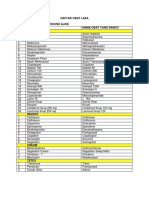
- Daftar Obat LasaDokumen2 halamanDaftar Obat LasaKhalifatus SaadahBelum ada peringkat
- Cefuroxime Drug Study ChanDokumen5 halamanCefuroxime Drug Study Chanczeremar chanBelum ada peringkat
- CNS Drug ListDokumen13 halamanCNS Drug ListAnaliza Kitongan LantayanBelum ada peringkat
- List of Selected Sanjeevini Combinations SSCDokumen1 halamanList of Selected Sanjeevini Combinations SSCsatyr7020% (1)
- Jurnal Referensi Zat BesiDokumen10 halamanJurnal Referensi Zat BesiChaerul TwentyOneBelum ada peringkat
- Model Answers Oet Official Writing PDFDokumen24 halamanModel Answers Oet Official Writing PDFTasneem Osman100% (1)
- Ceftriaxone RocephinDokumen1 halamanCeftriaxone RocephinEBelum ada peringkat
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDokumen45 halamanTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsBelum ada peringkat
- Maret 18 PDFDokumen178 halamanMaret 18 PDFAnonymous vLgCd0U7Belum ada peringkat
- Medicamentos Essenciais para Jovens MedicosDokumen2 halamanMedicamentos Essenciais para Jovens MedicosVieira MarceloBelum ada peringkat
- Online IVDrugChartDokumen23 halamanOnline IVDrugChartKenneth Remolete100% (1)
- Immunization Routine TableDokumen9 halamanImmunization Routine TablewenyinriantoBelum ada peringkat
- ClindamycinDokumen4 halamanClindamycinapi-37979410% (1)
- STG 2017 Final November 2017 PDF For SharingDokumen389 halamanSTG 2017 Final November 2017 PDF For SharingVitalis Mbuya100% (2)
- Cardiovascular Diseases AssignmentDokumen3 halamanCardiovascular Diseases AssignmentitziarccBelum ada peringkat
- Pharmacology Antibiotics: Fluoroquinolone - Chloramphenicol - TetracycllineDokumen40 halamanPharmacology Antibiotics: Fluoroquinolone - Chloramphenicol - TetracycllinemluthfidunandBelum ada peringkat
- Acute Abdomen During Pregnancy BelaynehDokumen47 halamanAcute Abdomen During Pregnancy BelaynehYohannis AsefaBelum ada peringkat
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaDokumen10 halamanFaktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaAsha NopatiBelum ada peringkat
- Co Amoxiclav (Broad Spectrum Penicillin)Dokumen3 halamanCo Amoxiclav (Broad Spectrum Penicillin)Danielle Marie SamblacenoBelum ada peringkat
- Vaccina1365tion FAQDokumen2 halamanVaccina1365tion FAQAtharvaBelum ada peringkat
- Peptic Ulcer: Nursing Case StudyDokumen21 halamanPeptic Ulcer: Nursing Case StudyRuhi ThakurBelum ada peringkat
- Chronic Kidney Disease LIFA FixxxDokumen19 halamanChronic Kidney Disease LIFA FixxxMuzdalifa MohamadBelum ada peringkat
- STD Comparison ChartDokumen5 halamanSTD Comparison ChartIvy Tee100% (2)