Anda mungkin juga menyukai
- 2013 He Zha LiDokumen10 halaman2013 He Zha LianuragBelum ada peringkat
- Audit Selection Strategy For Improving Tax Compliance - Application of Data Mining TechniquesDokumen10 halamanAudit Selection Strategy For Improving Tax Compliance - Application of Data Mining TechniquesanuragBelum ada peringkat
- Synergy Consulting Inc. Role Documentation - Master BookDokumen14 halamanSynergy Consulting Inc. Role Documentation - Master BookanuragBelum ada peringkat
- TM Dialling NoDokumen5 halamanTM Dialling NoKiran KumarBelum ada peringkat
- Synergy Consulting Inc. Role Documentation - Master BookDokumen14 halamanSynergy Consulting Inc. Role Documentation - Master BookanuragBelum ada peringkat
- Dissertation Project Work ListDokumen1 halamanDissertation Project Work ListanuragBelum ada peringkat
- Lagging Behind Zara and H&M in India, US Label Gap Finally Looks To Cut Prices by 10-15% - The Economic TimesDokumen2 halamanLagging Behind Zara and H&M in India, US Label Gap Finally Looks To Cut Prices by 10-15% - The Economic TimesanuragBelum ada peringkat
- Narayana HrudayalayaDokumen3 halamanNarayana Hrudayalayaanurag100% (1)
- Icici Bank Vodafone India Launch MpesaDokumen4 halamanIcici Bank Vodafone India Launch MpesaanuragBelum ada peringkat
- In TMT Future of e Commerce NoexpDokumen40 halamanIn TMT Future of e Commerce Noexpanurag100% (1)
- R&D Roadmap Blast FurnaceDokumen37 halamanR&D Roadmap Blast FurnaceVishal JainBelum ada peringkat
- Narayana HrudayalayaDokumen3 halamanNarayana Hrudayalayaanurag100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- NWH Hospitals Empanelled Under RBSK: Sl. No. Hospital Name Taluk DistrictDokumen3 halamanNWH Hospitals Empanelled Under RBSK: Sl. No. Hospital Name Taluk Districtraamki_99Belum ada peringkat
- NH Annual Report 2016 17 PDFDokumen260 halamanNH Annual Report 2016 17 PDFR.Rajalakshmi RajendranBelum ada peringkat
- Inventive IndianDokumen168 halamanInventive Indianvijay7775303Belum ada peringkat
- Narayana Hrudayalaya Hospitals Research PaperDokumen27 halamanNarayana Hrudayalaya Hospitals Research Paperapi-238825442Belum ada peringkat
- Narayana Hurdyalaya Business Model CanvasDokumen7 halamanNarayana Hurdyalaya Business Model CanvasShubham SinhaBelum ada peringkat
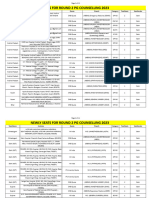
- Newly Seats For Round 2 PG Counselling 2023Dokumen11 halamanNewly Seats For Round 2 PG Counselling 2023Manoj KumarBelum ada peringkat
- 7p and 4i, NarayanaDokumen3 halaman7p and 4i, NarayanaVineet Pandey100% (1)
- Dr Devi Shetty on Affordable Healthcare SolutionsDokumen38 halamanDr Devi Shetty on Affordable Healthcare SolutionsVishwa SrivastavaBelum ada peringkat
- DETAILED PROJECT REPORT FOR OPERATION & MANAGEMENT SERVICES AT BHARUCH HOSPITALDokumen89 halamanDETAILED PROJECT REPORT FOR OPERATION & MANAGEMENT SERVICES AT BHARUCH HOSPITALzaheeruddin_mohdBelum ada peringkat
- NEET Super Speciality Counseling 2022 Round 1 Quota AbbreviationsDokumen208 halamanNEET Super Speciality Counseling 2022 Round 1 Quota AbbreviationsMinerva Medical Treatment Pvt LtdBelum ada peringkat
- Marketing AnalysisDokumen6 halamanMarketing AnalysisSwagato SarkarBelum ada peringkat
- Narayana Hrudalaya Heart HospitalDokumen17 halamanNarayana Hrudalaya Heart HospitalWaibhav Krishna100% (1)
- Narayana Hrudayalaya - 141215 PDFDokumen7 halamanNarayana Hrudayalaya - 141215 PDFrawatbs2020Belum ada peringkat
- Narayana HrudayalayaDokumen3 halamanNarayana Hrudayalayaanurag100% (1)
- Case 2 - Narayan HrudayalayaDokumen10 halamanCase 2 - Narayan Hrudayalayasujal vermaBelum ada peringkat
- DRAFT RED HERRING PROSPECTUS FOR NARAYANA HRUDAYALAYA IPODokumen548 halamanDRAFT RED HERRING PROSPECTUS FOR NARAYANA HRUDAYALAYA IPOShubham SinhaBelum ada peringkat
- Fixing - Nigeria (1) - 1 PDFDokumen40 halamanFixing - Nigeria (1) - 1 PDFFlying Doctors Nigeria100% (1)
- Devi ShettyDokumen38 halamanDevi ShettySujana RudrawaramBelum ada peringkat
- Narayana Hrudayalaya Corporate Overview and Vision to Become India's Largest Private Healthcare ProviderDokumen2 halamanNarayana Hrudayalaya Corporate Overview and Vision to Become India's Largest Private Healthcare ProviderChandra Sekhar100% (2)
- Axis Bank ListDokumen33 halamanAxis Bank ListNiketa OjhaBelum ada peringkat
- Post MBBS - Third Round Allotment DetailsDokumen89 halamanPost MBBS - Third Round Allotment DetailsAashish KapoorBelum ada peringkat
- Narayana HrudalayaDokumen20 halamanNarayana HrudalayaBikash Jaiswal100% (1)
- Narayan 2016Dokumen213 halamanNarayan 2016Jupe JonesBelum ada peringkat
- Company Profile Big BazaarDokumen17 halamanCompany Profile Big BazaarManikandan Mba0% (1)
- Peinv - Deals in PharmaDokumen9 halamanPeinv - Deals in PharmaSaurabh JainBelum ada peringkat
- On Narayana Hrudayalaya by Anup (Kumar OjhaDokumen10 halamanOn Narayana Hrudayalaya by Anup (Kumar Ojhaanupojha100% (2)
- Central Government Employees News - List of New Hospitals Empanelled Under CGHS, BengaluruDokumen7 halamanCentral Government Employees News - List of New Hospitals Empanelled Under CGHS, BengalururamanijiBelum ada peringkat
- Narayana Hrudayalaya - Section C - Group 5Dokumen22 halamanNarayana Hrudayalaya - Section C - Group 5raushanrahulBelum ada peringkat
- Narayana Hrudayalaya Cardiac Hospital Case Study LessonsDokumen11 halamanNarayana Hrudayalaya Cardiac Hospital Case Study LessonsSuhaib KhanBelum ada peringkat
- CGHS Empaneled HospitalsDokumen61 halamanCGHS Empaneled HospitalsAshutosh SaxenaBelum ada peringkat