Anda mungkin juga menyukai
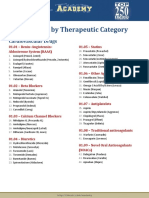
- Drug List by Therapeutic Category: Cardiovascular DrugsDokumen7 halamanDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Belum ada peringkat
- Pharmacological Classification of Drugs First EditionDokumen22 halamanPharmacological Classification of Drugs First EditionAsiya ZaidiBelum ada peringkat
- Pharmacological Classification of Drugs First EditionDokumen0 halamanPharmacological Classification of Drugs First EditionAmina BećiragićBelum ada peringkat
- 0194599812467004Dokumen55 halaman0194599812467004Asiya ZaidiBelum ada peringkat
- List of Drugs PDFDokumen59 halamanList of Drugs PDFLouriel Nopal100% (1)
- List of Books - Pharmacology TitlesDokumen2 halamanList of Books - Pharmacology TitlesAsiya ZaidiBelum ada peringkat
- CI ComparisonDokumen7 halamanCI ComparisonAsiya ZaidiBelum ada peringkat
- 0194599812467004Dokumen55 halaman0194599812467004Asiya ZaidiBelum ada peringkat
- 100 Cases in Ear, Nose & ThroatDokumen45 halaman100 Cases in Ear, Nose & Throatapi-3730930100% (17)
- Myringoplasty and TympanoplastyDokumen20 halamanMyringoplasty and TympanoplastyAsiya Zaidi100% (1)
- Foreign Body AspirationDokumen3 halamanForeign Body AspirationAsiya ZaidiBelum ada peringkat
- Cholesteatoma Pic 2013 05Dokumen90 halamanCholesteatoma Pic 2013 05Asiya ZaidiBelum ada peringkat
- Facial Paral Pic 2012 10 BDokumen70 halamanFacial Paral Pic 2012 10 BAsiya ZaidiBelum ada peringkat
- Reconstruction of Middle Ear CavityDokumen56 halamanReconstruction of Middle Ear CavityAsiya ZaidiBelum ada peringkat
- Ossicular Recon Slides 090629Dokumen89 halamanOssicular Recon Slides 090629Mohammed Sahib100% (1)
- Mastoidectomy and EpitympanectomyDokumen18 halamanMastoidectomy and EpitympanectomyAsiya ZaidiBelum ada peringkat
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDokumen9 halamanOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryAsiya ZaidiBelum ada peringkat
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDokumen9 halamanOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryAsiya ZaidiBelum ada peringkat
- Hoarse Lesion Slides 090306Dokumen61 halamanHoarse Lesion Slides 090306Asiya ZaidiBelum ada peringkat
- Classification of Hearing Loss PDFDokumen4 halamanClassification of Hearing Loss PDFAsiya ZaidiBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Limbah PabrikDokumen2 halamanLimbah Pabrikindar dewaBelum ada peringkat
- Artikel Ilmiah FikriDokumen6 halamanArtikel Ilmiah FikriViola Mei DamayantiBelum ada peringkat
- Turkey ImportDokumen14 halamanTurkey ImportMani 1Belum ada peringkat
- Refraction Through Lenses & Optical Instruments5Dokumen144 halamanRefraction Through Lenses & Optical Instruments5geniusamahBelum ada peringkat
- Large and Medium Manufacturing Industry Survey Report 2018Dokumen778 halamanLarge and Medium Manufacturing Industry Survey Report 2018melakuBelum ada peringkat
- Integrating Kuleana Rights and Land Trust PrioritesDokumen50 halamanIntegrating Kuleana Rights and Land Trust PrioritesKeala Rodenhurst-JamesBelum ada peringkat
- 1 s2.0 S2214860417301148 Main PDFDokumen16 halaman1 s2.0 S2214860417301148 Main PDFQuy Hoang KimBelum ada peringkat
- CERT Basic Training Participant Manual - 2011Dokumen332 halamanCERT Basic Training Participant Manual - 2011jegodfreyBelum ada peringkat
- Tiger 690 Conversion PDFDokumen8 halamanTiger 690 Conversion PDFGerardo Esteban Lagos RojasBelum ada peringkat
- Diff Types of Transmission Lines Used in CommsDokumen9 halamanDiff Types of Transmission Lines Used in CommsLe AndroBelum ada peringkat
- Carta Psicrometrica PDFDokumen2 halamanCarta Psicrometrica PDFJuliethBelum ada peringkat
- 2nd - Science-Second-Quarter-Week-1Dokumen37 halaman2nd - Science-Second-Quarter-Week-1Arlene AranzasoBelum ada peringkat
- Lession Plan - MIDokumen21 halamanLession Plan - MINithya SannidhiBelum ada peringkat
- Civil Eng Internship ReportDokumen6 halamanCivil Eng Internship ReportAromatic-O PBelum ada peringkat
- Dental Radiographs and Photographs in Human Forensic IdentificationDokumen8 halamanDental Radiographs and Photographs in Human Forensic IdentificationBudi PurnomoBelum ada peringkat
- Applied Acoustics: André M.N. Spillere, Augusto A. Medeiros, Julio A. CordioliDokumen13 halamanApplied Acoustics: André M.N. Spillere, Augusto A. Medeiros, Julio A. CordioliAbdelali MoumenBelum ada peringkat
- The Karnataka Maternity Benefit (Amendment) Rules 2019Dokumen30 halamanThe Karnataka Maternity Benefit (Amendment) Rules 2019Manisha SBelum ada peringkat
- Nest Installation GuideDokumen8 halamanNest Installation GuideOzzyBelum ada peringkat
- Man FXM FKM Motors PDFDokumen176 halamanMan FXM FKM Motors PDFRenato MeloBelum ada peringkat
- Infinera Product BrochureDokumen4 halamanInfinera Product Brochurebarry_fieldBelum ada peringkat
- General Psychology - Unit 2Dokumen23 halamanGeneral Psychology - Unit 2shivapriya ananthanarayananBelum ada peringkat
- Proceedings of National Conference on Landslides held in LudhianaDokumen8 halamanProceedings of National Conference on Landslides held in LudhianaAniket PawarBelum ada peringkat
- Consumer preference towards branded milk: A comparative analysis of Verka milk and Amul milkDokumen12 halamanConsumer preference towards branded milk: A comparative analysis of Verka milk and Amul milkBhawna RehanBelum ada peringkat
- Narayana Sukta MeaningDokumen4 halamanNarayana Sukta Meaningvinai.20Belum ada peringkat
- Analytical Mechanics SolutionsDokumen193 halamanAnalytical Mechanics SolutionsQuinton Boltin67% (9)
- PCS PADDLE SHIFTER INSTALL GUIDEDokumen21 halamanPCS PADDLE SHIFTER INSTALL GUIDEAndreas T P ManurungBelum ada peringkat
- Hyundai Elevator Manual Helmon 2000 InstructionDokumen27 halamanHyundai Elevator Manual Helmon 2000 InstructionReynold Suarez100% (1)
- Paradise Pools Flyer With Price ListDokumen5 halamanParadise Pools Flyer With Price ListKhuzaima HussainBelum ada peringkat
- Raspberry PiDokumen19 halamanRaspberry PiAnonymous E4Rbo2s100% (1)
- Warhammer 40k Kroot VehiclesDokumen2 halamanWarhammer 40k Kroot VehiclesJoseph RobinsonBelum ada peringkat