Anda mungkin juga menyukai
- Sleep-Related Headache and Its Management: Repalda, Myca Nicole D. BSN3Dokumen3 halamanSleep-Related Headache and Its Management: Repalda, Myca Nicole D. BSN3ampalBelum ada peringkat
- Analysing The Chart 1. Say What The Chart ShowsDokumen1 halamanAnalysing The Chart 1. Say What The Chart ShowsampalBelum ada peringkat
- Maternity NotificationDokumen2 halamanMaternity Notificationzacc83% (6)
- Jeep-Feb 26Dokumen1 halamanJeep-Feb 26ampalBelum ada peringkat
- Lucero, Diane A. Personality TestsDokumen3 halamanLucero, Diane A. Personality TestsampalBelum ada peringkat
- Status Epilepticus in AdultsDokumen3 halamanStatus Epilepticus in AdultsampalBelum ada peringkat
- Treatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodDokumen9 halamanTreatment of Classic Syndromes in Idiopathic Focal Epilepsies in ChildhoodampalBelum ada peringkat
- Drug Study NubainDokumen2 halamanDrug Study NubainampalBelum ada peringkat
- Convulsive Status Epilepticus N Children and Adults: Report of The Guideline Committee of The American Epilepsy Society. Retrieved FromDokumen1 halamanConvulsive Status Epilepticus N Children and Adults: Report of The Guideline Committee of The American Epilepsy Society. Retrieved FromampalBelum ada peringkat
- Krijrano G. Cabañez Bsnursing Iii: Sen A, Capelli V, Husain M (February, 2018)Dokumen3 halamanKrijrano G. Cabañez Bsnursing Iii: Sen A, Capelli V, Husain M (February, 2018)ampalBelum ada peringkat
- Epilepsy Status Epilepticus Headache: Submitted By: Yzrah Duffnee Dezz P. Mangubat BS Nursing - IiiDokumen1 halamanEpilepsy Status Epilepticus Headache: Submitted By: Yzrah Duffnee Dezz P. Mangubat BS Nursing - IiiampalBelum ada peringkat
- Preoperative Information Needs of Children Undergoing TonsillectomyDokumen1 halamanPreoperative Information Needs of Children Undergoing TonsillectomyampalBelum ada peringkat
- Pathophysiology of AsthmaDokumen1 halamanPathophysiology of AsthmaampalBelum ada peringkat
- Maam Intong Journal ArticleDokumen1 halamanMaam Intong Journal ArticleampalBelum ada peringkat
- Letter HospitalDokumen2 halamanLetter HospitalampalBelum ada peringkat
- Scleroderma PathophysiologyDokumen3 halamanScleroderma PathophysiologyampalBelum ada peringkat
- Journal For or Workbook 2Dokumen1 halamanJournal For or Workbook 2ampalBelum ada peringkat
- The World Health OrganizationDokumen4 halamanThe World Health Organizationampal100% (1)
- Systemic Lupus ErythematousDokumen8 halamanSystemic Lupus ErythematousampalBelum ada peringkat
- Republic of The PhilippinesDokumen2 halamanRepublic of The PhilippinesampalBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Chapter 3Dokumen3 halamanChapter 3Htet_Aung_HlaingBelum ada peringkat
- January 2011 MS - Unit 1 WJEC Physics A-LevelDokumen4 halamanJanuary 2011 MS - Unit 1 WJEC Physics A-Levelfadi baqainBelum ada peringkat
- Electricity An SmagnetismDokumen2 halamanElectricity An SmagnetismRonit BiswalBelum ada peringkat
- Case Study Class 9Dokumen4 halamanCase Study Class 9JAYA BALDEV DasBelum ada peringkat
- Living SystemsDokumen45 halamanLiving SystemslorettaensBelum ada peringkat
- Class IX (Physics) Unit-1-Edited PDFDokumen96 halamanClass IX (Physics) Unit-1-Edited PDFKanhaiya Kumar JhaBelum ada peringkat
- Experiment 3: Conditions For EquilibriumDokumen8 halamanExperiment 3: Conditions For EquilibriumToni Andrei CervalesBelum ada peringkat
- S. C. Bott Et Al - Study of The Effect of Current Rise Time On The Formation of The Precursor Column in Cylindrical Wire Array Z Pinches at 1 MADokumen14 halamanS. C. Bott Et Al - Study of The Effect of Current Rise Time On The Formation of The Precursor Column in Cylindrical Wire Array Z Pinches at 1 MACola7890Belum ada peringkat
- T Are A Potencial Electrico 2016Dokumen4 halamanT Are A Potencial Electrico 2016Servando De La CruzBelum ada peringkat
- CH 7 System of ParticlesDokumen25 halamanCH 7 System of ParticlesazeenBelum ada peringkat
- Worksheet - M1 - AnswersDokumen4 halamanWorksheet - M1 - AnswersGhBelum ada peringkat
- Stage 2 Biomechanics 2nd Ed Sample PackageDokumen13 halamanStage 2 Biomechanics 2nd Ed Sample PackagegundadanBelum ada peringkat
- 11th Physics Book Back Questions With Answers in EnglishDokumen29 halaman11th Physics Book Back Questions With Answers in EnglishsuryaBelum ada peringkat
- Motion in A Straight LineDokumen26 halamanMotion in A Straight LineLord Siva100% (3)
- Student Exploration: Weight and MassDokumen4 halamanStudent Exploration: Weight and MasskeymariBelum ada peringkat
- Electric Field Intensity and Potintials.Dokumen17 halamanElectric Field Intensity and Potintials.Prudhvi Raghu TejaBelum ada peringkat
- DYNAMICSDokumen15 halamanDYNAMICSElisante ManguBelum ada peringkat
- Chapter 2 - DynamicsDokumen8 halamanChapter 2 - DynamicsTHIÊN LÊ TRẦN THUẬNBelum ada peringkat
- Simple Machines Unit PlanDokumen7 halamanSimple Machines Unit PlanthisjimithingBelum ada peringkat
- FrictionDokumen31 halamanFrictionSarilyn Simon50% (4)
- Population Pie ChartDokumen6 halamanPopulation Pie ChartCzantal Ruth Naomi GarciaBelum ada peringkat
- E mc2 - Google SearchDokumen1 halamanE mc2 - Google Searchmbeee6ixtee01Belum ada peringkat
- Relativistic EffectsDokumen16 halamanRelativistic EffectsQasim AliBelum ada peringkat
- Chapter 2-Phy220Dokumen55 halamanChapter 2-Phy220Jordan TuckerBelum ada peringkat
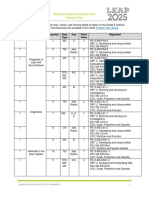
- Leap 2025 Grade 6 Science Practice Test Answer KeyDokumen38 halamanLeap 2025 Grade 6 Science Practice Test Answer KeyTrisha ManaloBelum ada peringkat
- X. Rotational Equilibrium and Rotational DynamicsDokumen17 halamanX. Rotational Equilibrium and Rotational DynamicsPatrick SibandaBelum ada peringkat
- Perhitungan Kuat Tekan WFDokumen7 halamanPerhitungan Kuat Tekan WFYoni Ardianto PrabowoBelum ada peringkat
- Multiple Choice Questions Carry: StationaryDokumen13 halamanMultiple Choice Questions Carry: StationaryDuo Genius- Physics Wallah Inspired100% (1)
- Lecture Planner - Physics - PW Vidyapeeth School 11th JEE (Alpha)Dokumen3 halamanLecture Planner - Physics - PW Vidyapeeth School 11th JEE (Alpha)Divyanshu JethwaniBelum ada peringkat
- Class 11 Physics (Set - A)Dokumen7 halamanClass 11 Physics (Set - A)Teri MeriBelum ada peringkat