Anda mungkin juga menyukai
- 2-6 Book-2Dokumen400 halaman2-6 Book-2Drx ahmed MaherBelum ada peringkat
- RecertificationDokumen10 halamanRecertificationDrx ahmed MaherBelum ada peringkat
- Presentation TipsDokumen4 halamanPresentation TipsDrx ahmed MaherBelum ada peringkat
- Candidates GuideDokumen17 halamanCandidates GuideDrx ahmed MaherBelum ada peringkat
- Types of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDokumen48 halamanTypes of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDrx ahmed MaherBelum ada peringkat
- Able of Ontents: EdiatricsDokumen4 halamanAble of Ontents: EdiatricsDrx ahmed MaherBelum ada peringkat
- Types of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDokumen48 halamanTypes of Economic and Humanistic Outcomes Assessments: Kathleen M. Bungay, Pharm.D. and Lisa A. Sanchez, Pharm.DDrx ahmed MaherBelum ada peringkat
- 080 2Dokumen28 halaman080 2Drx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen34 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- 070 2Dokumen31 halaman070 2Drx ahmed MaherBelum ada peringkat
- 080 3Dokumen44 halaman080 3Drx ahmed MaherBelum ada peringkat
- 050 3Dokumen22 halaman050 3Drx ahmed MaherBelum ada peringkat
- 070 1Dokumen24 halaman070 1Drx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen21 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- 060 3Dokumen35 halaman060 3Drx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: Endocrine and Metabolic DisordersDokumen32 halamanConflict of Interest Disclosures: Endocrine and Metabolic DisordersDrx ahmed MaherBelum ada peringkat
- 2011 Updates in Therapeutics:: Conflict of Interest DisclosuresDokumen14 halaman2011 Updates in Therapeutics:: Conflict of Interest DisclosuresDrx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen34 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- Conflict of Interest DisclosuresDokumen24 halamanConflict of Interest DisclosuresDrx ahmed MaherBelum ada peringkat
- 050 1Dokumen38 halaman050 1Drx ahmed MaherBelum ada peringkat
- 040 2Dokumen26 halaman040 2Drx ahmed MaherBelum ada peringkat
- 2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDokumen11 halaman2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDrx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen39 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- 040 1Dokumen44 halaman040 1Drx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen39 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- OutlineDokumen20 halamanOutlineDrx ahmed MaherBelum ada peringkat
- OutlineDokumen20 halamanOutlineDrx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosure: 2011 Updates in TherapeuticsDokumen19 halamanConflict of Interest Disclosure: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- Conflict of Interest Disclosures: 2011 Updates in TherapeuticsDokumen24 halamanConflict of Interest Disclosures: 2011 Updates in TherapeuticsDrx ahmed MaherBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Institute of Ergonomics Human Factors. Conference PDFDokumen632 halamanInstitute of Ergonomics Human Factors. Conference PDFIngrid BeatrixBelum ada peringkat
- CdcmmwrreportDokumen116 halamanCdcmmwrreportapi-235277923Belum ada peringkat
- Pembimbing: Dr. Yanto Budiman, Sp. Rad, M.Kes Presentan: Handy Putra 2010.061.006 Melissa Nathania Theda 2010.061.007 Stefanus Harris 2010.061.014Dokumen49 halamanPembimbing: Dr. Yanto Budiman, Sp. Rad, M.Kes Presentan: Handy Putra 2010.061.006 Melissa Nathania Theda 2010.061.007 Stefanus Harris 2010.061.014yani_utBelum ada peringkat
- Tenopa 60SC MSDSDokumen8 halamanTenopa 60SC MSDSSadhana SentosaBelum ada peringkat
- AnatomyDokumen2 halamanAnatomymhredBelum ada peringkat
- Medication Errors & AdrDokumen6 halamanMedication Errors & AdrMEERA HOSPITALBelum ada peringkat
- Pub Fetal-Mri PDFDokumen543 halamanPub Fetal-Mri PDFAndreea RoxanaBelum ada peringkat
- Chapter 05: Selecting The Ventilator and The ModeDokumen13 halamanChapter 05: Selecting The Ventilator and The Modespace100% (1)
- GreenKInd Magazine, Vol 2, No 2Dokumen46 halamanGreenKInd Magazine, Vol 2, No 2GREEN KIND MAGAZINEBelum ada peringkat
- Ivermectin: Paste 1 .87%Dokumen1 halamanIvermectin: Paste 1 .87%JuanBelum ada peringkat
- Consultants PDFDokumen21 halamanConsultants PDFMartin RongenBelum ada peringkat
- DETOX WATERS FOR GLOWING SKINDokumen18 halamanDETOX WATERS FOR GLOWING SKINsandeep swamyBelum ada peringkat
- Dentaltown 2018marchDokumen113 halamanDentaltown 2018marchDanutz BalanBelum ada peringkat
- Antidepression Reiki PDFDokumen6 halamanAntidepression Reiki PDFKamlesh Mehta100% (2)
- ld50 LabDokumen6 halamanld50 Labapi-277689164Belum ada peringkat
- FCPS Part 1 Ophthalmology Nov 2012 Review (40chDokumen13 halamanFCPS Part 1 Ophthalmology Nov 2012 Review (40chbahaashakirBelum ada peringkat
- Hypothyroidism (Myxedema)Dokumen25 halamanHypothyroidism (Myxedema)Arzo AnumBelum ada peringkat
- 10 11648 J SJPH S 2015030501 21Dokumen6 halaman10 11648 J SJPH S 2015030501 21Muhammad FakhriBelum ada peringkat
- 140b-56109667-Standing Supported Left Glute Push Clinical ReasoningDokumen2 halaman140b-56109667-Standing Supported Left Glute Push Clinical ReasoningAbhishek VermaBelum ada peringkat
- PRC Schedule Licensure Exam 2020Dokumen7 halamanPRC Schedule Licensure Exam 2020TheSummitExpress50% (2)
- Nursing Documentation and ReportingDokumen0 halamanNursing Documentation and ReportingJames Avoka Asamani83% (6)
- Australian Clinical Psychosis GuidelinesDokumen18 halamanAustralian Clinical Psychosis Guidelinessolomon1234567Belum ada peringkat
- Interventional NeuroradiologyDokumen442 halamanInterventional NeuroradiologyBagus Ngurah MahasenaBelum ada peringkat
- Biodentine A Promising Dentin Substitute Jimds 1000140Dokumen5 halamanBiodentine A Promising Dentin Substitute Jimds 1000140MihEugenBelum ada peringkat
- Asia Pacific Obesity 2000Dokumen56 halamanAsia Pacific Obesity 2000Melissa SindiongBelum ada peringkat
- Bluvias and Eckert Sea Turtle Husbandry Manual 2010Dokumen108 halamanBluvias and Eckert Sea Turtle Husbandry Manual 2010Hazel LopezBelum ada peringkat
- Sejarah Dan Definisi Psikologi PositifDokumen11 halamanSejarah Dan Definisi Psikologi PositifHaryadi KurniawanBelum ada peringkat
- Capstone PaperDokumen8 halamanCapstone Paperapi-260053520Belum ada peringkat
- EID JournalDokumen175 halamanEID JournalArthur Boegaurd100% (1)
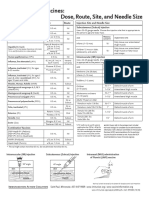
- Injection Site and Needle Size Vaccine Dose RouteDokumen1 halamanInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaBelum ada peringkat