Anda mungkin juga menyukai
- Understanding Acute and Chronic LeukemiaDokumen10 halamanUnderstanding Acute and Chronic LeukemiaKrisha BalorioBelum ada peringkat
- Medical certificate from Pantalan SHSDokumen2 halamanMedical certificate from Pantalan SHSAngelo Villafranca67% (3)
- Hangnails and HomoeopathyDokumen7 halamanHangnails and HomoeopathyDr. Rajneesh Kumar Sharma MD HomBelum ada peringkat
- Interpretting ABG SuccessfullyDokumen15 halamanInterpretting ABG Successfullyanimathz100% (1)
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDokumen9 halamanAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiBelum ada peringkat
- Fast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsDari EverandFast Facts: Measurable Residual Disease: A clearer picture for treatment decisionsBelum ada peringkat
- Recall 3Dokumen22 halamanRecall 3Christine Rodriguez-Guerrero100% (4)
- By S.Dharaniya, 3 Year BiotechnologyDokumen14 halamanBy S.Dharaniya, 3 Year BiotechnologyrevaishBelum ada peringkat
- Sysemic Lupus Erythematosus Case StudyDokumen53 halamanSysemic Lupus Erythematosus Case StudyJennylen Torres100% (1)
- Blood Bank ChecklistDokumen4 halamanBlood Bank ChecklistFIAZ MAQBOOL FAZILIBelum ada peringkat
- ANA Patterns EuroimmuneDokumen4 halamanANA Patterns EuroimmuneManuel ArenasBelum ada peringkat
- Ana & Its InterpretationDokumen48 halamanAna & Its InterpretationSiddharth DashBelum ada peringkat
- Atlas of Antinuclear AntibodiesDokumen40 halamanAtlas of Antinuclear AntibodiesFAIZAN KHANBelum ada peringkat
- ASCP Recalls and Lab Tests GuideDokumen22 halamanASCP Recalls and Lab Tests Guidebaihern24Belum ada peringkat
- Antinuclear Antibodies Marker of Diagnosis and Evolution in Autoimmune DiseasesDokumen12 halamanAntinuclear Antibodies Marker of Diagnosis and Evolution in Autoimmune DiseasesFAIZAN KHANBelum ada peringkat
- Atlas Patrones ANADokumen56 halamanAtlas Patrones ANAkemitaBelum ada peringkat
- Standardised ANA Pattern ClassificationDokumen4 halamanStandardised ANA Pattern ClassificationLucia OlosuteanBelum ada peringkat
- Lo Coco FrancescoDokumen61 halamanLo Coco FrancescoJess silvaBelum ada peringkat
- Ana TestDokumen4 halamanAna TestFariz NurBelum ada peringkat
- Lecture6 - Personalized Genomics 2019Dokumen208 halamanLecture6 - Personalized Genomics 2019Charlie HouBelum ada peringkat
- Evaluation and Comparison of Three Assays For Molecular Detection of Spinal Muscular AtrophyDokumen11 halamanEvaluation and Comparison of Three Assays For Molecular Detection of Spinal Muscular AtrophyRainie PhamBelum ada peringkat
- Jurnal SLEDokumen7 halamanJurnal SLEDevinta NauraBelum ada peringkat
- AutoantibodiesDokumen13 halamanAutoantibodiesCristina ElenaBelum ada peringkat
- ANA TestDokumen16 halamanANA TestSami Al WesabiBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen14 halamanNIH Public Access: Author ManuscriptAlejandra BonillaBelum ada peringkat
- FULL-2225 - Intermediate LearningDokumen9 halamanFULL-2225 - Intermediate LearningNaziBrola TsivadzeBelum ada peringkat
- Interpreting Anti HLA Antibody Testing Data A.14Dokumen10 halamanInterpreting Anti HLA Antibody Testing Data A.14MARIA LEIVABelum ada peringkat
- Auto Antibody Testing For Autoimmune DiseaseDokumen8 halamanAuto Antibody Testing For Autoimmune DiseaseDaniel MoránBelum ada peringkat
- Antinuclear Antibody ANADokumen3 halamanAntinuclear Antibody ANAanaelisabetapBelum ada peringkat
- Fibra PequeñaDokumen7 halamanFibra PequeñaPile BallBelum ada peringkat
- HDTD-B-10 - Molecular Genetics IIDokumen40 halamanHDTD-B-10 - Molecular Genetics IIMariam QaisBelum ada peringkat
- Revision Tut 3 Block 1Dokumen11 halamanRevision Tut 3 Block 1Matsiri ImmanuelBelum ada peringkat
- Unknown Author - AutoantibodypdfDokumen7 halamanUnknown Author - AutoantibodypdfBhupi AgrawalBelum ada peringkat
- CT of Central Nervous System Infections in Immunocompromised PatientsDokumen5 halamanCT of Central Nervous System Infections in Immunocompromised PatientsRe-zha 'Putra'Belum ada peringkat
- Circulating NAD+ Metabolism-Derived Genes Unveils Prognostic and Peripheral Immune Infiltration in Amyotrophic Lateral SclerosisDokumen14 halamanCirculating NAD+ Metabolism-Derived Genes Unveils Prognostic and Peripheral Immune Infiltration in Amyotrophic Lateral SclerosisCVAS-007 College Of Veterinary And Animal Sciences, JhangBelum ada peringkat
- 2018 Oh LabMedOnlineDokumen4 halaman2018 Oh LabMedOnlineEduardo PasteneBelum ada peringkat
- Sysmex Xtra XS Series Outstanding X-Class TechnologyDokumen5 halamanSysmex Xtra XS Series Outstanding X-Class TechnologyKhashayar ModaberiBelum ada peringkat
- Assessment of Antinuclear Antibodies (ANA) National Recommendations OnDokumen20 halamanAssessment of Antinuclear Antibodies (ANA) National Recommendations Onmilica cucuzBelum ada peringkat
- ASL Perfusion of The Brain Emerging Clinical ApplicationDokumen20 halamanASL Perfusion of The Brain Emerging Clinical ApplicationpoppyBelum ada peringkat
- Antinuclear Antibody Test: KeywordsDokumen4 halamanAntinuclear Antibody Test: KeywordsInmunoquímica CP BiomédicosBelum ada peringkat
- The Neutrophil Lymphocyte Ratio Consideracoes para Aplicacoes ClinicasDokumen2 halamanThe Neutrophil Lymphocyte Ratio Consideracoes para Aplicacoes Clinicasbrunareis1999Belum ada peringkat
- Ernst - KDM4C in JAK2-Mutated Neoplasms, Leukemia, 2022Dokumen7 halamanErnst - KDM4C in JAK2-Mutated Neoplasms, Leukemia, 2022Beatriz Garcia RiartBelum ada peringkat
- FINAL Neuroendocrine TumoursDokumen35 halamanFINAL Neuroendocrine Tumoursabhinav_choudhary03Belum ada peringkat
- Laboratory Tests in Hematological Malignancies 2Dokumen40 halamanLaboratory Tests in Hematological Malignancies 2Abdulelah MurshidBelum ada peringkat
- Connective Tissue DZDokumen1 halamanConnective Tissue DZAndre GarciaBelum ada peringkat
- Write 1Dokumen6 halamanWrite 1Mehedi HossainBelum ada peringkat
- Ferroptosis: An Iron-Dependent Form of Regulated Cell DeathDokumen11 halamanFerroptosis: An Iron-Dependent Form of Regulated Cell DeathLaura MarcelaBelum ada peringkat
- From Ana To EnaDokumen8 halamanFrom Ana To EnaJasBelum ada peringkat
- Journal of Musculoskeletal Disorders and Treatment JMDT 6 080 PDFDokumen7 halamanJournal of Musculoskeletal Disorders and Treatment JMDT 6 080 PDFMarvin Josue Bustamante GutierrezBelum ada peringkat
- Autoimmune Vestibulocerebellar SyndromesDokumen19 halamanAutoimmune Vestibulocerebellar Syndromesrafael rocha novaesBelum ada peringkat
- ANA Patterns 5Dokumen1 halamanANA Patterns 5renee iiiBelum ada peringkat
- Characterization Ribdnucleoprotein AutoantigenDokumen9 halamanCharacterization Ribdnucleoprotein AutoantigenLe DungBelum ada peringkat
- Bi Omar CadresDokumen33 halamanBi Omar CadresNataly Butrón BustamanteBelum ada peringkat
- Paraneoplastic Disorders of the Central Nervous SystemDokumen71 halamanParaneoplastic Disorders of the Central Nervous Systempreeti sharmaBelum ada peringkat
- Autoimmune Encephalitis: ClinicalperspectivesDokumen10 halamanAutoimmune Encephalitis: ClinicalperspectivesNatalia Gutierrez MarchenaBelum ada peringkat
- MCTD 3Dokumen1 halamanMCTD 3Laksmita Ayu Dewi TetanelBelum ada peringkat
- Huang 2021Dokumen7 halamanHuang 2021Lucas AmorimBelum ada peringkat
- Buka Lit (4) SDokumen21 halamanBuka Lit (4) SArumm88Belum ada peringkat
- Detecting and Quantifying Ischemic Stroke on CTDokumen26 halamanDetecting and Quantifying Ischemic Stroke on CTGabriella ALeBelum ada peringkat
- Urja Synopsis - Final FDokumen47 halamanUrja Synopsis - Final Fforam patelBelum ada peringkat
- 10 1016@j Ajhg 2019 04 014Dokumen8 halaman10 1016@j Ajhg 2019 04 014Ifany oschaliaBelum ada peringkat
- Recognition and Relevance of Anti-Dfs70 Autoantibodies in Routine Antinuclear Autoantibodies Testing at A Community HospitalDokumen9 halamanRecognition and Relevance of Anti-Dfs70 Autoantibodies in Routine Antinuclear Autoantibodies Testing at A Community HospitalirsyadilfikriBelum ada peringkat
- 10 1002@ana 25083Dokumen56 halaman10 1002@ana 25083Mickola VorokhtaBelum ada peringkat
- Diagnostic Testing and Interpretation of Tests ForDokumen10 halamanDiagnostic Testing and Interpretation of Tests ForPuri RahmawatiBelum ada peringkat
- (Kasus-Endokrin) (2016!11!10) A Management of Type 2 Diabetes Mellitus and Hyperglycemic Hyperosmolar State in A Patient With Pulmonary Tuberculosis (Ismayadi)Dokumen11 halaman(Kasus-Endokrin) (2016!11!10) A Management of Type 2 Diabetes Mellitus and Hyperglycemic Hyperosmolar State in A Patient With Pulmonary Tuberculosis (Ismayadi)Fariz NurBelum ada peringkat
- Pathophysiology of AKI BasileDokumen99 halamanPathophysiology of AKI BasileFariz NurBelum ada peringkat
- 2015 AHA Guidelines Highlights EnglishDokumen36 halaman2015 AHA Guidelines Highlights EnglishshiloinBelum ada peringkat
- Respiratory Tract InfectionDokumen13 halamanRespiratory Tract InfectionFariz NurBelum ada peringkat
- Fatal Leptopsirosis CaseDokumen6 halamanFatal Leptopsirosis CaseFariz NurBelum ada peringkat
- Guidelines For The Prevention, Care And... Ic Hepatitis B PDFDokumen16 halamanGuidelines For The Prevention, Care And... Ic Hepatitis B PDFFariz NurBelum ada peringkat
- Ana TestDokumen4 halamanAna TestFariz NurBelum ada peringkat
- Frailty, John E. MorleyDokumen11 halamanFrailty, John E. MorleyFariz NurBelum ada peringkat
- Neutrophil GranulocyteDokumen16 halamanNeutrophil GranulocyteFariz NurBelum ada peringkat
- Respiratory Tract InfectionDokumen13 halamanRespiratory Tract InfectionFariz NurBelum ada peringkat
- Activation of The Coagulation Cascade in Patients With LeptospirosisDokumen7 halamanActivation of The Coagulation Cascade in Patients With LeptospirosisFariz NurBelum ada peringkat
- Ethionamide-Induced Hypothyroidism in ChildrenDokumen3 halamanEthionamide-Induced Hypothyroidism in ChildrenFariz NurBelum ada peringkat
- Di, Siadh, CSWDokumen17 halamanDi, Siadh, CSWVanitha Ratha KrishnanBelum ada peringkat
- En Wikipedia Org Wiki Absolute Neutrophil CountDokumen5 halamanEn Wikipedia Org Wiki Absolute Neutrophil CountFariz NurBelum ada peringkat
- Di, Siadh, CSWDokumen17 halamanDi, Siadh, CSWVanitha Ratha KrishnanBelum ada peringkat
- H.pylori Dan CA GasterDokumen32 halamanH.pylori Dan CA GasterFariz NurBelum ada peringkat
- Ethionamide-Induced Hypothyroidism in ChildrenDokumen3 halamanEthionamide-Induced Hypothyroidism in ChildrenFariz NurBelum ada peringkat
- En Wikipedia Org Wiki Absolute Neutrophil CountDokumen5 halamanEn Wikipedia Org Wiki Absolute Neutrophil CountFariz NurBelum ada peringkat
- Death Fariz 2-1-14Dokumen5 halamanDeath Fariz 2-1-14Fariz NurBelum ada peringkat
- Insiden RematologiDokumen11 halamanInsiden RematologiFariz NurBelum ada peringkat
- Understanding The Epidemiology SleDokumen12 halamanUnderstanding The Epidemiology SleFariz NurBelum ada peringkat
- Hyperbaric Oxygen Therapy: ReferenceDokumen5 halamanHyperbaric Oxygen Therapy: ReferenceFariz NurBelum ada peringkat
- Ajg 1998292 ADokumen9 halamanAjg 1998292 AFariz NurBelum ada peringkat
- Steroid Lupus NefritisDokumen3 halamanSteroid Lupus NefritisFariz NurBelum ada peringkat
- Bacterial factors and host immune responses in H pylori infectionDokumen5 halamanBacterial factors and host immune responses in H pylori infectionFariz NurBelum ada peringkat
- Helicobacter Pylori Eradication: Changes in Gastric Acid Secretion Assayed by Endoscopic Gastrin Test Before and AfterDokumen7 halamanHelicobacter Pylori Eradication: Changes in Gastric Acid Secretion Assayed by Endoscopic Gastrin Test Before and AfterFariz NurBelum ada peringkat
- Ptre HT and MortalitasDokumen15 halamanPtre HT and MortalitasFariz NurBelum ada peringkat
- Hyperbaric Oxygen Therapy: ReferenceDokumen5 halamanHyperbaric Oxygen Therapy: ReferenceFariz NurBelum ada peringkat
- Factors Associated With ParadoxicalDokumen11 halamanFactors Associated With ParadoxicalFariz NurBelum ada peringkat
- Anterior Cruciate Ligament InjuryDokumen3 halamanAnterior Cruciate Ligament InjuryAdrian Nazario PragachaBelum ada peringkat
- Akupresur Point Hugo Mengurangi Nyeri Tusukan AVF pada Pasien HemodialisaDokumen10 halamanAkupresur Point Hugo Mengurangi Nyeri Tusukan AVF pada Pasien HemodialisamargaretBelum ada peringkat
- Hip Dislocation ResearchDokumen8 halamanHip Dislocation Researchapi-268839011Belum ada peringkat
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDokumen8 halamanVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengBelum ada peringkat
- It 18 - Neonatal Seizure - HerDokumen35 halamanIt 18 - Neonatal Seizure - HerRurie Awalia SuhardiBelum ada peringkat
- Prostaglandins: An Overview of Structure and FunctionDokumen33 halamanProstaglandins: An Overview of Structure and FunctionMuhammad JamalBelum ada peringkat
- A Case Report On Sickle Cell Disease With Hemolyti PDFDokumen4 halamanA Case Report On Sickle Cell Disease With Hemolyti PDFAlhaji SwarrayBelum ada peringkat
- Triage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDDokumen6 halamanTriage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDRatna SariBelum ada peringkat
- Periapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesDokumen9 halamanPeriapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesFlorin Ionescu100% (1)
- Resume - Viroja Sweta For PortfolioDokumen1 halamanResume - Viroja Sweta For Portfolioapi-608195339Belum ada peringkat
- Understanding Traumatic Brain Injury (TBIDokumen16 halamanUnderstanding Traumatic Brain Injury (TBIdcBelum ada peringkat
- Sleep and The Risk of Chronic Kidney Disease: A Cohort StudyDokumen8 halamanSleep and The Risk of Chronic Kidney Disease: A Cohort StudyEtaursaeBelum ada peringkat
- CNA Chapter 1 & 2 TermsDokumen1 halamanCNA Chapter 1 & 2 TermsMarina ChakarBelum ada peringkat
- Smart + Smart Enhancer: Medic MedicDokumen11 halamanSmart + Smart Enhancer: Medic MedicmiazainuddinBelum ada peringkat
- 7-Physiology of Normal PuerperiumDokumen24 halaman7-Physiology of Normal Puerperiumhade elBelum ada peringkat
- Mini-implant molar intrusion caseDokumen1 halamanMini-implant molar intrusion caseVesna AndreevskaBelum ada peringkat
- Urinary System Disorders Practice Quiz #1 (50 Questions)Dokumen26 halamanUrinary System Disorders Practice Quiz #1 (50 Questions)Emy TandinganBelum ada peringkat
- National Institute of Occupational Safety and Health Course CurriculumDokumen9 halamanNational Institute of Occupational Safety and Health Course Curriculummohan dassBelum ada peringkat
- Body's Battles (gnv64) PDFDokumen96 halamanBody's Battles (gnv64) PDFameyparanjape100% (1)
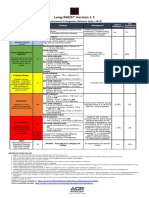
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- Multiple PregnancyDokumen16 halamanMultiple Pregnancyjane7arian7berzabalBelum ada peringkat
- Uncorrected Author ProofDokumen15 halamanUncorrected Author ProofindahBelum ada peringkat
- Infectiile Grave Extensive Ale Partilor MoiDokumen49 halamanInfectiile Grave Extensive Ale Partilor MoiLoredana BoghezBelum ada peringkat
- Audiometric Evaluation Report .: Left Ear Right EarDokumen1 halamanAudiometric Evaluation Report .: Left Ear Right EarRaja IsaacBelum ada peringkat
- C-Section Guide: What to Expect with Cesarean DeliveryDokumen3 halamanC-Section Guide: What to Expect with Cesarean DeliveryFEALABREPORTSBelum ada peringkat