Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- WHO Systems Thinking 9789241563895 - EngDokumen112 halamanWHO Systems Thinking 9789241563895 - EngCraig Dalton100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Useful Phrases For Writing EssaysDokumen4 halamanUseful Phrases For Writing EssaysAlexander Zeus100% (3)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- UtilitarianismDokumen6 halamanUtilitarianismRanz GieoBelum ada peringkat
- R&D Tax CreditDokumen7 halamanR&D Tax Creditb_tallerBelum ada peringkat
- Pead 3 - Abdominal Pain and VommitingDokumen22 halamanPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Henri J. M. Nouwen, "Celibacy" (1978)Dokumen12 halamanHenri J. M. Nouwen, "Celibacy" (1978)JonathanBelum ada peringkat
- Ra 6981Dokumen17 halamanRa 6981Michelle Quiquino FolienteBelum ada peringkat
- Harley Merlin 6 - Harley Merlin and The Cult of ErisDokumen343 halamanHarley Merlin 6 - Harley Merlin and The Cult of ErisSOUFIANE RACHID83% (6)
- CONSTI 2 Midterm PointersDokumen10 halamanCONSTI 2 Midterm PointersRommel P. Abas100% (1)
- Advanced Life Support AssessmentDokumen1 halamanAdvanced Life Support AssessmentbbyesBelum ada peringkat
- Pead 1 - NeonatologyDokumen21 halamanPead 1 - NeonatologybbyesBelum ada peringkat
- Early Pregnancy ComplciationsDokumen43 halamanEarly Pregnancy ComplciationsbbyesBelum ada peringkat
- Tocolytics in PretermDokumen13 halamanTocolytics in PretermbbyesBelum ada peringkat
- BASIC Course Gosford June 2021Dokumen3 halamanBASIC Course Gosford June 2021bbyesBelum ada peringkat
- Guideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisDokumen18 halamanGuideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisbbyesBelum ada peringkat
- Substance Abuse in PregnancyDokumen151 halamanSubstance Abuse in PregnancybbyesBelum ada peringkat
- Prenatal ScreeningDokumen26 halamanPrenatal ScreeningbbyesBelum ada peringkat
- C SpineDokumen44 halamanC SpinebbyesBelum ada peringkat
- Position Description ENTDokumen3 halamanPosition Description ENTbbyesBelum ada peringkat
- SSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExamDokumen4 halamanSSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExambbyesBelum ada peringkat
- HMO Surgical PositionDokumen4 halamanHMO Surgical PositionbbyesBelum ada peringkat
- Surgical - Information GuideDokumen2 halamanSurgical - Information GuidebbyesBelum ada peringkat
- Ischkwa DiagramDokumen1 halamanIschkwa DiagrambbyesBelum ada peringkat
- Training Manual 2020Dokumen53 halamanTraining Manual 2020bbyesBelum ada peringkat
- Organisation Chart - TraineeDokumen1 halamanOrganisation Chart - TraineebbyesBelum ada peringkat
- ECGs - UpdatedDokumen26 halamanECGs - UpdatedbbyesBelum ada peringkat
- Right VATS Pleural BiopsyDokumen4 halamanRight VATS Pleural BiopsybbyesBelum ada peringkat
- RHDDokumen130 halamanRHDDeepu RajendranBelum ada peringkat
- Upper GI BleedDokumen8 halamanUpper GI BleedbbyesBelum ada peringkat
- Atrial Fibrillation Managing Acute Atrial FibrillationDokumen8 halamanAtrial Fibrillation Managing Acute Atrial FibrillationbbyesBelum ada peringkat
- Varicose VeinDokumen6 halamanVaricose VeinbbyesBelum ada peringkat
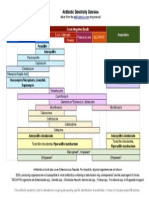
- Antibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesDokumen1 halamanAntibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesGuillermo Damian RodriguezBelum ada peringkat
- Infections in PregnancyDokumen11 halamanInfections in PregnancybbyesBelum ada peringkat
- Pump Manual TextDokumen17 halamanPump Manual TextbbyesBelum ada peringkat
- Shoulder PainDokumen5 halamanShoulder PainbbyesBelum ada peringkat
- Weekly SDS Topics: Week 3Dokumen1 halamanWeekly SDS Topics: Week 3bbyesBelum ada peringkat
- Prof PracDokumen3 halamanProf PracbbyesBelum ada peringkat
- Main Presentations of Sexually Transmitted Infections in MenDokumen3 halamanMain Presentations of Sexually Transmitted Infections in MenbbyesBelum ada peringkat
- Midterm 2 Enculturation and SocializationDokumen56 halamanMidterm 2 Enculturation and SocializationMa Kaycelyn SayasBelum ada peringkat
- Critical Reading and Writing For PostgraduatesDokumen5 halamanCritical Reading and Writing For PostgraduatesNmushaikwaBelum ada peringkat
- INTL711 Introduction Week 7 Entrepreneurship, Innovation, and Economic Development PDFDokumen31 halamanINTL711 Introduction Week 7 Entrepreneurship, Innovation, and Economic Development PDFAnonymous I03Wesk92Belum ada peringkat
- Personal Details Form.v5.0Dokumen2 halamanPersonal Details Form.v5.0LoBelum ada peringkat
- Once There Lived A Young Merchant Named Ivan Dmitri Aksenov With His Family in The Land of VladimirDokumen5 halamanOnce There Lived A Young Merchant Named Ivan Dmitri Aksenov With His Family in The Land of VladimirCharles M. MartinBelum ada peringkat
- CBBL01 eDokumen1 halamanCBBL01 ejoanna supresenciaBelum ada peringkat
- IntroductionDokumen28 halamanIntroductionPushpa BaruaBelum ada peringkat
- Logical Framework Analysis ToolDokumen8 halamanLogical Framework Analysis Toolabh1sh3kBelum ada peringkat
- FERHANE Cherazade - Charles Martin in UgandaDokumen4 halamanFERHANE Cherazade - Charles Martin in UgandaJuliop Cangry RamosBelum ada peringkat
- Covid Letter and Consent FormDokumen2 halamanCovid Letter and Consent FormBATMANBelum ada peringkat
- Tamilmani - Resume 2021 PDFDokumen4 halamanTamilmani - Resume 2021 PDFTitan TamilBelum ada peringkat
- Measuring Performance & Managing ResultsDokumen4 halamanMeasuring Performance & Managing ResultsParveen MaanBelum ada peringkat
- Assessment 2Dokumen9 halamanAssessment 2api-486388549Belum ada peringkat
- Legal OpinionDokumen3 halamanLegal OpinionGilgoric NgohoBelum ada peringkat
- The Goose GirlDokumen2 halamanThe Goose Girlapi-235508995Belum ada peringkat
- Use A Single Space 12-Point Font When Writing. Your Assignment Should Be About 1100+ WordsDokumen7 halamanUse A Single Space 12-Point Font When Writing. Your Assignment Should Be About 1100+ WordsRaman RandhawaBelum ada peringkat
- Transfer of Property Act - Ramesh Chand Vs Suresh Chand, Delhi High CourtDokumen18 halamanTransfer of Property Act - Ramesh Chand Vs Suresh Chand, Delhi High CourtLatest Laws TeamBelum ada peringkat
- Exercise No. 5Dokumen1 halamanExercise No. 5Princess Therese CañeteBelum ada peringkat
- International Strategies Group, LTD v. Greenberg Traurig, LLP Et Al - Document No. 10Dokumen3 halamanInternational Strategies Group, LTD v. Greenberg Traurig, LLP Et Al - Document No. 10Justia.comBelum ada peringkat
- Supreme Court Judgment on Land Acquisition ProceedingsDokumen35 halamanSupreme Court Judgment on Land Acquisition ProceedingsRishabh BhargavaBelum ada peringkat
- 5 BPI Family Bank Vs FrancoDokumen15 halaman5 BPI Family Bank Vs FrancoSDN HelplineBelum ada peringkat
- Crim 1 CasesDokumen228 halamanCrim 1 CasesLeo Mark LongcopBelum ada peringkat