Anda mungkin juga menyukai
- SOCIETY For ENDOCRINOLOGY ENDOCRINE EMERGENCY GUIDANCE - Emergency Management of Acute Adrenal Insufficiency (Adrenal Crisis) in Adult PatientsDokumen3 halamanSOCIETY For ENDOCRINOLOGY ENDOCRINE EMERGENCY GUIDANCE - Emergency Management of Acute Adrenal Insufficiency (Adrenal Crisis) in Adult PatientsMuhammad ReyhanBelum ada peringkat
- Wounds in GeneralDokumen19 halamanWounds in GeneralMuhammad ReyhanBelum ada peringkat
- Radiological Signs of Lobar Collapse. Chest Radiographic Findings and CT ImagesDokumen38 halamanRadiological Signs of Lobar Collapse. Chest Radiographic Findings and CT ImagesMuhammad ReyhanBelum ada peringkat
- Exercise and Older Patients - Prescribing Guidelines PDFDokumen8 halamanExercise and Older Patients - Prescribing Guidelines PDFMuhammad ReyhanBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Tablas de Presión ArterialDokumen2 halamanTablas de Presión Arterialwasserpura100% (1)
- Dicionario NihonDokumen10 halamanDicionario NihonMario GuedesBelum ada peringkat
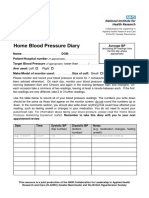
- Home Blood Pressure DiaryDokumen2 halamanHome Blood Pressure DiaryCherieBelum ada peringkat
- 2015 Book HandbookOfCardiacAnatomyPhysio PDFDokumen806 halaman2015 Book HandbookOfCardiacAnatomyPhysio PDFChema Sánchez100% (2)
- Project #7 - HypertensionDokumen2 halamanProject #7 - HypertensionKPBelum ada peringkat
- Ezpap - Effects of EzPAP Post Operatively in Coronary Artery Bypass Graft PatientsDokumen1 halamanEzpap - Effects of EzPAP Post Operatively in Coronary Artery Bypass Graft Patientsjesushenandez_ftrBelum ada peringkat
- STENTSDokumen260 halamanSTENTSRoberto J. Santos RibeiroBelum ada peringkat
- Rules For EKG StripsDokumen5 halamanRules For EKG StripsjessiBelum ada peringkat
- 30 Dec JoBs BY KHALIQ HASSAN - Watermarked PDFDokumen4 halaman30 Dec JoBs BY KHALIQ HASSAN - Watermarked PDFKamran Talpur100% (1)
- Department of Internal Medicine: Manila Doctors HospitalDokumen5 halamanDepartment of Internal Medicine: Manila Doctors HospitalFayeListanco100% (1)
- 2015 American Heart Association Guidelines Update For CPR and ECCDokumen32 halaman2015 American Heart Association Guidelines Update For CPR and ECCVauFauziah100% (2)
- Tetralogy of FallotDokumen18 halamanTetralogy of FallotAaronMaroonFive100% (1)
- Mitral Valve Disease Information Sheet-1Dokumen6 halamanMitral Valve Disease Information Sheet-1Ionela OprescuBelum ada peringkat
- Blood Pressure ChartDokumen5 halamanBlood Pressure ChartAnonymous LiddTaTaZTBelum ada peringkat
- Echocardiographic Features of Total Anomalous Pulmonary: VenousDokumen8 halamanEchocardiographic Features of Total Anomalous Pulmonary: VenousTanuj VermaBelum ada peringkat
- Diabetes and HypertensionDokumen196 halamanDiabetes and HypertensionMed Aj100% (1)
- Drugs Affecting BPDokumen36 halamanDrugs Affecting BPm1k0eBelum ada peringkat
- Allen: Transportation in Plants and AnimalsDokumen12 halamanAllen: Transportation in Plants and AnimalsAnant DwivediBelum ada peringkat
- MRCP Passmedicine Part II 2017Dokumen8.783 halamanMRCP Passmedicine Part II 2017Prakash MahatoBelum ada peringkat
- Case Presentation 2Dokumen27 halamanCase Presentation 2Sathish SPBelum ada peringkat
- Neonatal Life Support UK Ressusstation Council G2015 - NLSDokumen1 halamanNeonatal Life Support UK Ressusstation Council G2015 - NLSBharat Kumar SharmaBelum ada peringkat
- Lec Activity11 and 13 Blood Blood VesselDokumen2 halamanLec Activity11 and 13 Blood Blood Vesselapple BananaBelum ada peringkat
- Catheter Ablation For Atrial Fibrillation: Original ArticleDokumen7 halamanCatheter Ablation For Atrial Fibrillation: Original ArticleGavin WinkelBelum ada peringkat
- Vena Contracta Width Is A Semi-Quantitative Parameter To Assess The Severity of Mitral RegurgitationDokumen20 halamanVena Contracta Width Is A Semi-Quantitative Parameter To Assess The Severity of Mitral Regurgitationalex leeBelum ada peringkat
- HypoxemiaDokumen3 halamanHypoxemiaMark Angelo ChanBelum ada peringkat
- Normal ECGDokumen2 halamanNormal ECGGeneon100% (1)
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDokumen9 halamanHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenBelum ada peringkat
- Essentials of Cardiopulmonary Physical Therapy 4th Edition Hillegass Test BankDokumen10 halamanEssentials of Cardiopulmonary Physical Therapy 4th Edition Hillegass Test Banknancycarrollaocprizwen100% (9)
- Dental Management Medically Compromised Patient 9th Little Test BankDokumen5 halamanDental Management Medically Compromised Patient 9th Little Test BankSaifoqq100% (1)
- Post-Test - Google FormsDokumen18 halamanPost-Test - Google FormsTrixia AlmendralBelum ada peringkat