Anda mungkin juga menyukai
- Early Language Milestone Scale 2Dokumen1 halamanEarly Language Milestone Scale 2Ronald Ivan WijayaBelum ada peringkat
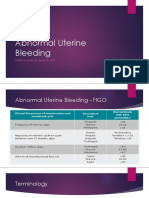
- Abnormal Uterine BleedingDokumen33 halamanAbnormal Uterine BleedingGregorius Juan GunawanBelum ada peringkat
- Uterine Bleeding-A Case StudyDokumen4 halamanUterine Bleeding-A Case StudyRoanne Lagua0% (1)
- Dysfunctional: Articles BleedingDokumen5 halamanDysfunctional: Articles BleedingMonika JonesBelum ada peringkat
- Artículo Menopausia 2Dokumen17 halamanArtículo Menopausia 2daniela otaBelum ada peringkat
- Postmenopausal Bleeding - StatPearls - NCBI BooksDokumen11 halamanPostmenopausal Bleeding - StatPearls - NCBI BooksKalaivathanan VathananBelum ada peringkat
- AFP Abnormal MensesDokumen12 halamanAFP Abnormal Mensespatrick_raj884545Belum ada peringkat
- 11abnormal Uterine BleedingDokumen32 halaman11abnormal Uterine BleedingAkinbani MoyosoreBelum ada peringkat
- 16 Prolapse IndonesianDokumen17 halaman16 Prolapse IndonesianDwi MahendraBelum ada peringkat
- Abnormaluterinebleeding: Ashraf Khafaga,, Steven R. GoldsteinDokumen11 halamanAbnormaluterinebleeding: Ashraf Khafaga,, Steven R. GoldsteinEvelyn Pamela Espinoza MoralesBelum ada peringkat
- The Evaluation of Abnormal Uterine BleedingDokumen16 halamanThe Evaluation of Abnormal Uterine BleedingEstefania gonzalez torresBelum ada peringkat
- Abnormal Uterine BleedingDokumen11 halamanAbnormal Uterine BleedingKharmell Waters AndradeBelum ada peringkat
- Dysfunctional Uterine Bleeding: Clinical UpdateDokumen3 halamanDysfunctional Uterine Bleeding: Clinical Updateragil putra jBelum ada peringkat
- Dysfunctional Uterine Bleeding: Prepared By: Sabnam Gurung Roll No:31Dokumen39 halamanDysfunctional Uterine Bleeding: Prepared By: Sabnam Gurung Roll No:31Sabnam GurungBelum ada peringkat
- Abnormal Uterine BleedingDokumen7 halamanAbnormal Uterine BleedingBrian Fry100% (1)
- Abnormal Uterine BleedingDokumen23 halamanAbnormal Uterine BleedingTakeru Ferry100% (2)
- Abnormal Uterine BleedingDokumen23 halamanAbnormal Uterine BleedingTakeru Ferry100% (1)
- Abnormal Uterine Bleeding in The Adolescent CME 2020Dokumen7 halamanAbnormal Uterine Bleeding in The Adolescent CME 2020Mariana HernandezBelum ada peringkat
- Abnormal Bleeding in AdolescentDokumen7 halamanAbnormal Bleeding in AdolescentRosa AlvaradoBelum ada peringkat
- Practice: Dysfunctional Uterine BleedingDokumen2 halamanPractice: Dysfunctional Uterine Bleedingragil putra jBelum ada peringkat
- Pages From FEB 2020 WH Assessment 1Dokumen5 halamanPages From FEB 2020 WH Assessment 12019B-03Mailani NisyraBelum ada peringkat
- ACOG 2011 Management of The Adnexal Mass June 2011Dokumen16 halamanACOG 2011 Management of The Adnexal Mass June 2011Arlen Patricia Soto LópezBelum ada peringkat
- Abnormal Uterine BleedingDokumen64 halamanAbnormal Uterine BleedingAakriti GargBelum ada peringkat
- Clinical Features of MyomasDokumen16 halamanClinical Features of MyomasMona HelouBelum ada peringkat
- Abnormal Uterine BleedingDokumen5 halamanAbnormal Uterine Bleedingmendato marcabanBelum ada peringkat
- Gynecology Abnormal Bleeding 2014aDokumen8 halamanGynecology Abnormal Bleeding 2014aBhi-An BatobalonosBelum ada peringkat
- Abnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarDokumen80 halamanAbnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarSharoon KumarBelum ada peringkat
- Dub Munro 2001Dokumen15 halamanDub Munro 2001IEKEBelum ada peringkat
- Abnormal Uterine BleedingDokumen36 halamanAbnormal Uterine BleedingPranshu Prajyot 67100% (1)
- Mohand XDokumen13 halamanMohand XakhomanBelum ada peringkat
- Management of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesDokumen4 halamanManagement of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesIda_Maryani94Belum ada peringkat
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueDokumen12 halamanBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriBelum ada peringkat
- 1.AUB (ESS) Final Ppt. DR - Ei Shwe SynDokumen44 halaman1.AUB (ESS) Final Ppt. DR - Ei Shwe SynYudha KhusniaBelum ada peringkat
- International Journal of Pharmaceutical Science Invention (IJPSI)Dokumen3 halamanInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsBelum ada peringkat
- Yale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1Dokumen12 halamanYale - Abnormal Uterine Bleeding Preceptor - 389620 - 284 - 45546 - v1omegasauron0gmailcomBelum ada peringkat
- Guidelines of Investigations of Premenopausal Women With Abnormal Uterine Bleeding - 2020Dokumen6 halamanGuidelines of Investigations of Premenopausal Women With Abnormal Uterine Bleeding - 2020cara0319Belum ada peringkat
- Long 1996Dokumen3 halamanLong 1996galihBelum ada peringkat
- Sangrado Uterino en UrgenciaDokumen13 halamanSangrado Uterino en UrgenciaVictoria Oliva ZúñigaBelum ada peringkat
- Clinical: Section 3 of 10Dokumen36 halamanClinical: Section 3 of 10coleBelum ada peringkat
- ACOG Abnormal Uterine Bleeding DiagnosisDokumen11 halamanACOG Abnormal Uterine Bleeding DiagnosisJimmy Crack CornsBelum ada peringkat
- Adenomyosis: Student PresentationDokumen19 halamanAdenomyosis: Student PresentationRae RayBelum ada peringkat
- Dysfunctional Uterine BleedingDokumen7 halamanDysfunctional Uterine BleedingNhorz Love UBelum ada peringkat
- Practice Bulletin: Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged WomenDokumen10 halamanPractice Bulletin: Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged WomenJuwita Valen RamadhanniaBelum ada peringkat
- Abnormal Uterine Bleeding in Premenopausal Women: Co Pyr Igh TDokumen3 halamanAbnormal Uterine Bleeding in Premenopausal Women: Co Pyr Igh TFebrina Sylva FridayantiBelum ada peringkat
- CE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFDokumen5 halamanCE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFrizqina ajraBelum ada peringkat
- Jay BagrateeDokumen49 halamanJay BagrateeirmaarmiyahBelum ada peringkat
- Abnormal Uterine BleedingDokumen2 halamanAbnormal Uterine BleedingeinlancherBelum ada peringkat
- Endometrial Study by TVS and It's Correlation With Histopathology in Abnormal Uterine BleedingDokumen12 halamanEndometrial Study by TVS and It's Correlation With Histopathology in Abnormal Uterine BleedingIOSRjournalBelum ada peringkat
- Abnormal Uterine Bleeding in A 39 Year OldDokumen16 halamanAbnormal Uterine Bleeding in A 39 Year OldEliana GerzonBelum ada peringkat
- Abnormal Uterine BleedingDokumen9 halamanAbnormal Uterine BleedingMahmudi .nur19Belum ada peringkat
- Captura de Pantalla 2024-04-06 A La(s) 0.37.53Dokumen14 halamanCaptura de Pantalla 2024-04-06 A La(s) 0.37.53miguelangulo63557Belum ada peringkat
- Features Concerning For Significant Pathology Prompting Early Referral IncludeDokumen5 halamanFeatures Concerning For Significant Pathology Prompting Early Referral IncludeNatalita ChristianiBelum ada peringkat
- Incidence of Endometrial Hyperplasia in 100 Cases Presenting With Polymenorrhagia/Menorrhagia in Perimenupausal WomenDokumen4 halamanIncidence of Endometrial Hyperplasia in 100 Cases Presenting With Polymenorrhagia/Menorrhagia in Perimenupausal Womenfitrah fajrianiBelum ada peringkat
- Aub Management AlgorithmDokumen13 halamanAub Management AlgorithmsugiartixBelum ada peringkat
- Abnormal Uterine Bleeding in Perimenopausal WomenDokumen15 halamanAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandBelum ada peringkat
- IJOGR 6 3 308 31120200528 47399 FVXWQK With Cover Page v2Dokumen5 halamanIJOGR 6 3 308 31120200528 47399 FVXWQK With Cover Page v2niningariestiBelum ada peringkat
- Uterine Bleeding: How Understanding Endometrial Physiology Underpins Menstrual HealthDokumen19 halamanUterine Bleeding: How Understanding Endometrial Physiology Underpins Menstrual Healthannisa lailaBelum ada peringkat
- Common Problems in Women S Health 19Dokumen33 halamanCommon Problems in Women S Health 19afifahsalsabilaaaBelum ada peringkat
- Gynecologic Pain and Vaginal Bleeding: Jamie L. Collings and Nicholas A. BormDokumen11 halamanGynecologic Pain and Vaginal Bleeding: Jamie L. Collings and Nicholas A. BormAnton ArifinBelum ada peringkat
- Yale Curriculum ResourceDokumen10 halamanYale Curriculum ResourceGhazal KangoBelum ada peringkat
- Frozen Section Pathology: Diagnostic ChallengesDari EverandFrozen Section Pathology: Diagnostic ChallengesAlain C. BorczukBelum ada peringkat
- Simple List AlphaDokumen42 halamanSimple List AlphaRonald Ivan WijayaBelum ada peringkat
- RFD Fenol PDFDokumen30 halamanRFD Fenol PDFRonald Ivan WijayaBelum ada peringkat
- Msds PDFDokumen6 halamanMsds PDFEko SumiyantoBelum ada peringkat
- Acute MedicineDokumen321 halamanAcute MedicineMontasir Ahmed100% (18)
- Ni Seb Metallo Anti Malaria LsDokumen13 halamanNi Seb Metallo Anti Malaria LsRonald Ivan WijayaBelum ada peringkat
- RFC CO PDFDokumen7 halamanRFC CO PDFRonald Ivan WijayaBelum ada peringkat
- RFD Fenol PDFDokumen30 halamanRFD Fenol PDFRonald Ivan WijayaBelum ada peringkat
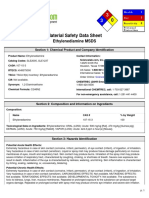
- MSDS Etilen DiaminDokumen6 halamanMSDS Etilen DiamindoubleyujeiBelum ada peringkat
- Experiment Distillation Limonene Completa Di TeoriaDokumen5 halamanExperiment Distillation Limonene Completa Di TeoriaRonald Ivan WijayaBelum ada peringkat
- Adl Adaptive Skill Checklist For 3 To 5 YearsDokumen2 halamanAdl Adaptive Skill Checklist For 3 To 5 YearsRonald Ivan WijayaBelum ada peringkat
- Ipi363073 PDFDokumen9 halamanIpi363073 PDFIndahSriWahyuniBelum ada peringkat
- Mutation Breeding: Taryono Faculty of Agriculture Gadjah Mada UniversityDokumen29 halamanMutation Breeding: Taryono Faculty of Agriculture Gadjah Mada UniversityRonald Ivan WijayaBelum ada peringkat
- Cover BrantsDokumen1 halamanCover BrantsRonald Ivan WijayaBelum ada peringkat
- 2104 Meningoencephalitis Due To Enteroviral Infection An Often Overlooked EtiologyDokumen4 halaman2104 Meningoencephalitis Due To Enteroviral Infection An Often Overlooked EtiologyRonald Ivan WijayaBelum ada peringkat
- Cover MullerDokumen1 halamanCover MullerRonald Ivan WijayaBelum ada peringkat
- Search Engine For Life-Science PDFs - PubgetDokumen2 halamanSearch Engine For Life-Science PDFs - PubgetRonald Ivan WijayaBelum ada peringkat
- Jact 06 I 3 P 225Dokumen11 halamanJact 06 I 3 P 225ferianaBelum ada peringkat
- Monteggia FractureDokumen11 halamanMonteggia FractureRonald Ivan WijayaBelum ada peringkat
- Post-Traumatic Stress Disorder - Theory - Pathophysiology - Best Practice - EnglishDokumen1 halamanPost-Traumatic Stress Disorder - Theory - Pathophysiology - Best Practice - EnglishRonald Ivan WijayaBelum ada peringkat
- J Neurol Neurosurg Psychiatry 2004 Kennedy I10 5Dokumen7 halamanJ Neurol Neurosurg Psychiatry 2004 Kennedy I10 5Ronald Ivan WijayaBelum ada peringkat
- Etyo & ClassifiDokumen3 halamanEtyo & ClassifiRonald Ivan WijayaBelum ada peringkat
- MagnesiumDokumen9 halamanMagnesiumBobanBisercicBelum ada peringkat
- Mechanism of InjuryDokumen3 halamanMechanism of InjuryRonald Ivan WijayaBelum ada peringkat
- Effects and Complications of Unilateral Spinalanesthesia Versus Standard Spinal Anesthesia in Lower-Limborthopedic SurgeryDokumen4 halamanEffects and Complications of Unilateral Spinalanesthesia Versus Standard Spinal Anesthesia in Lower-Limborthopedic SurgeryRonald Ivan WijayaBelum ada peringkat
- Efectos Postfertilizacion de DIU PDFDokumen10 halamanEfectos Postfertilizacion de DIU PDFRonald Ivan WijayaBelum ada peringkat
- Stress Response in Surgery and TraumaDokumen9 halamanStress Response in Surgery and TraumaLee June LyngBelum ada peringkat
- Treatment and ComplicationDokumen19 halamanTreatment and ComplicationRonald Ivan WijayaBelum ada peringkat
- The IUD: A Contraceptive Option For Postpartum and Postabortion WomenDokumen3 halamanThe IUD: A Contraceptive Option For Postpartum and Postabortion WomenRonald Ivan WijayaBelum ada peringkat
- 2-Pengaruh Konseling KB THD Kontrasepsi Iud Post-Chandradewi Ekayani SopiatunDokumen6 halaman2-Pengaruh Konseling KB THD Kontrasepsi Iud Post-Chandradewi Ekayani SopiatunRiniez Scatzy Ciimenirr YPasBelum ada peringkat
- Case Study in Architectural Structures: A-7E Avionics System - ADokumen36 halamanCase Study in Architectural Structures: A-7E Avionics System - Ajckz8Belum ada peringkat
- Operator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpDokumen12 halamanOperator'S Manual PM20X-X-X-BXX: 2" Diaphragm PumpOmar TadeoBelum ada peringkat
- Book of IQ TestsDokumen124 halamanBook of IQ TestsFox Mango100% (4)
- Routine Maintenance For External Water Tank Pump and Circulation Pump On FID Tower and Rack 2017-014Dokumen5 halamanRoutine Maintenance For External Water Tank Pump and Circulation Pump On FID Tower and Rack 2017-014CONVIERTE PDF JPG WORDBelum ada peringkat
- Ducati WiringDokumen7 halamanDucati WiringRyan LeisBelum ada peringkat
- R, Axn: Housingand RegulatoryDokumen5 halamanR, Axn: Housingand RegulatoryAce RamosoBelum ada peringkat
- Hydrogen Production by Steam ReformingDokumen10 halamanHydrogen Production by Steam ReformingramiarenasBelum ada peringkat
- Hatayoga 1Dokumen11 halamanHatayoga 1SACHIDANANDA SBelum ada peringkat
- DILG Opinion-Sanggunian Employees Disbursements, Sign Checks & Travel OrderDokumen2 halamanDILG Opinion-Sanggunian Employees Disbursements, Sign Checks & Travel OrderCrizalde de DiosBelum ada peringkat
- Region: South Central State: Andhra PradeshDokumen118 halamanRegion: South Central State: Andhra PradeshpaulinBelum ada peringkat
- Altos Easystore Users ManualDokumen169 halamanAltos Easystore Users ManualSebBelum ada peringkat
- Listening Tests 81112Dokumen13 halamanListening Tests 81112luprof tpBelum ada peringkat
- Aashirwaad Notes For CA IPCC Auditing & Assurance by Neeraj AroraDokumen291 halamanAashirwaad Notes For CA IPCC Auditing & Assurance by Neeraj AroraMohammed NasserBelum ada peringkat
- Load Schedule: DescriptionDokumen1 halamanLoad Schedule: Descriptionkurt james alorroBelum ada peringkat
- Paper 4 Material Management Question BankDokumen3 halamanPaper 4 Material Management Question BankDr. Rakshit Solanki100% (2)
- DXFtoGerberConversionGuide Rev2!12!10 13Dokumen8 halamanDXFtoGerberConversionGuide Rev2!12!10 13Tomasz BarwińskiBelum ada peringkat
- Poka-Yoke or Mistake Proofing: Historical Evolution.Dokumen5 halamanPoka-Yoke or Mistake Proofing: Historical Evolution.Harris ChackoBelum ada peringkat
- Context in TranslationDokumen23 halamanContext in TranslationRaluca FloreaBelum ada peringkat
- EvolutionCombatMedic 2022Dokumen17 halamanEvolutionCombatMedic 2022smith.kevin1420344100% (1)
- Types of Intermolecular ForcesDokumen34 halamanTypes of Intermolecular ForcesRuschan JaraBelum ada peringkat
- Most Probable Number (MPN) Test: Principle, Procedure, ResultsDokumen4 halamanMost Probable Number (MPN) Test: Principle, Procedure, ResultsHammad KingBelum ada peringkat
- Lesson 23 Career PathwaysDokumen34 halamanLesson 23 Career PathwaysAlfredo ModestoBelum ada peringkat
- Retailing PPT (Shailwi Nitish)Dokumen14 halamanRetailing PPT (Shailwi Nitish)vinit PatidarBelum ada peringkat
- Mongodb TutorialDokumen106 halamanMongodb TutorialRahul VashishthaBelum ada peringkat
- (Kazantzakis Nikos) Freedom or DeathDokumen195 halaman(Kazantzakis Nikos) Freedom or DeathTarlan FisherBelum ada peringkat
- Preblending of Raw Materia1Dokumen26 halamanPreblending of Raw Materia1Mohammed Abdo100% (1)
- Vtoris 100% Clean Paypal Transfer Guide 2015Dokumen8 halamanVtoris 100% Clean Paypal Transfer Guide 2015Sean FrohmanBelum ada peringkat
- Tutorial 3 MFRS8 Q PDFDokumen3 halamanTutorial 3 MFRS8 Q PDFKelvin LeongBelum ada peringkat
- Manual TV Hyundai HYLED3239iNTMDokumen40 halamanManual TV Hyundai HYLED3239iNTMReinaldo TorresBelum ada peringkat
- Annex A - Scope of WorkDokumen4 halamanAnnex A - Scope of Workمهيب سعيد الشميريBelum ada peringkat