Anda mungkin juga menyukai
- Ventura County Medical Center: Mi Thrombolysis, Management ofDokumen3 halamanVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657Belum ada peringkat
- Chest Pain Notes USMLE Step 3Dokumen3 halamanChest Pain Notes USMLE Step 3kisria100% (1)
- Rhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Dokumen10 halamanRhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Luis PadillaBelum ada peringkat
- St-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielDokumen28 halamanSt-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielLloyd Daniel BarrantesBelum ada peringkat
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDokumen6 halamanAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyBelum ada peringkat
- Clinical Learning Session-Acute Coronary Syndromes Acs - 1Dokumen31 halamanClinical Learning Session-Acute Coronary Syndromes Acs - 1api-611918048Belum ada peringkat
- Cme Acs 2. Stemi (Izzah)Dokumen36 halamanCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiBelum ada peringkat
- Acute Coronary Syndromes - HandoutDokumen4 halamanAcute Coronary Syndromes - Handoutapi-641524095Belum ada peringkat
- 49-Year-Old Male Admitted with Decreased SensoriumDokumen8 halaman49-Year-Old Male Admitted with Decreased SensoriumJan Crizza Dale R. FrancoBelum ada peringkat
- Arrhythmias EmergencyDokumen10 halamanArrhythmias EmergencyNITACORDEIROBelum ada peringkat
- Acute Stroke ProtocolDokumen3 halamanAcute Stroke ProtocolKarissaBelum ada peringkat
- Tatalaksana ArrthytmiaDokumen55 halamanTatalaksana ArrthytmiaJanstine FirstiandyBelum ada peringkat
- Acs CCS 2021 KLDokumen52 halamanAcs CCS 2021 KLPitchya WangmeesriBelum ada peringkat
- Treatment Protocol of SnakebiteDokumen23 halamanTreatment Protocol of SnakebiteEduconsultBelum ada peringkat
- Pre EclampsiaDokumen9 halamanPre EclampsiaAnixa GutiérrezBelum ada peringkat
- ACS ChartDokumen1 halamanACS ChartJoey TingBelum ada peringkat
- Acute Coronary SyndromesDokumen7 halamanAcute Coronary SyndromesOwen J. WieseBelum ada peringkat
- TPA Protocol: Stroke in Carefully Selected PersonsDokumen4 halamanTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMBelum ada peringkat
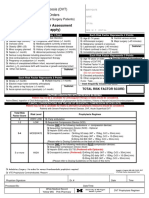
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDokumen2 halamanThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaBelum ada peringkat
- OSCE EmergencyDokumen26 halamanOSCE EmergencyXu PeihaoBelum ada peringkat
- CardiovascularDokumen23 halamanCardiovascularzacks nyirongoBelum ada peringkat
- Crisis of Hypertension Revised 1Dokumen57 halamanCrisis of Hypertension Revised 1keenmunir100% (4)
- ParulDokumen7 halamanParulПарул КатіярBelum ada peringkat
- ACLS ACS Algorithm NewDokumen3 halamanACLS ACS Algorithm Newsambo100% (1)
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Dokumen9 halamanO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasBelum ada peringkat
- TachycardiaDokumen7 halamanTachycardiaArvind SahniBelum ada peringkat
- NSTEMI Management: MHAM-College of MedicineDokumen14 halamanNSTEMI Management: MHAM-College of MedicineMykki Gigi NateBelum ada peringkat
- Acute Coronary SyndromeDokumen5 halamanAcute Coronary Syndromem3d1k100% (1)
- Treatment of Prolonged SeizuresDokumen1 halamanTreatment of Prolonged SeizuresAhmad ShukriBelum ada peringkat
- Kegawatan Jantung - MeDokumen41 halamanKegawatan Jantung - MeNam Min BinBelum ada peringkat
- Tatalaksana STEMI: Rizky Ramadhan N, DR RS Jampang KulonDokumen17 halamanTatalaksana STEMI: Rizky Ramadhan N, DR RS Jampang KulonRizky Ramadhan NuriaBelum ada peringkat
- AcsDokumen20 halamanAcsTitanSeptiansyahBelum ada peringkat
- The PatientDokumen9 halamanThe PatientJan Crizza Dale R. FrancoBelum ada peringkat
- Nstemi 3MBDokumen69 halamanNstemi 3MBDBelum ada peringkat
- Thrombolytic TherapyDokumen16 halamanThrombolytic TherapyAnonymous nrZXFwBelum ada peringkat
- Myocardial InfarctionDokumen39 halamanMyocardial InfarctionYauffa Hanna Elt MisykahBelum ada peringkat
- Supraventricular TachycardiaDokumen7 halamanSupraventricular Tachycardiaagarrido2Belum ada peringkat
- Acute Myocardial InfarctionDokumen13 halamanAcute Myocardial InfarctionSajjad KabirBelum ada peringkat
- Thrombolysis Version 2 0 2015 Final PDFDokumen16 halamanThrombolysis Version 2 0 2015 Final PDFtitisBelum ada peringkat
- Symptom Onset Arrival: Circle Yes, No or Not Known As AppropriateDokumen2 halamanSymptom Onset Arrival: Circle Yes, No or Not Known As AppropriateB-win IrawanBelum ada peringkat
- Fac Thrombolysis 2007Dokumen36 halamanFac Thrombolysis 2007Tri Harjono0% (1)
- Traumatic Brain Injury 2023Dokumen17 halamanTraumatic Brain Injury 2023Fernando Martinez AguilarBelum ada peringkat
- Acute Coronary Syndrome Acute MIDokumen41 halamanAcute Coronary Syndrome Acute MIAmjad SobehBelum ada peringkat
- 11-Acs2 StemiDokumen33 halaman11-Acs2 Stemiمحمد بن الصادقBelum ada peringkat
- ACLS Simulation ScenariosDokumen14 halamanACLS Simulation ScenariosVanessa HermioneBelum ada peringkat
- Perfusion, Class 11 ReviewedDokumen45 halamanPerfusion, Class 11 ReviewedMelissa GPBelum ada peringkat
- ACLS Algorithms Adult 2010 Revised May 31 2011Dokumen12 halamanACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614Belum ada peringkat
- Cardiology SBIM Part 1Dokumen14 halamanCardiology SBIM Part 1Gousay AlkhazmariBelum ada peringkat
- Strokes Student HandoutDokumen4 halamanStrokes Student HandoutMiss LindiweBelum ada peringkat
- Treatment Protocol of Snake Bite: Kaushik.H.M 080201388Dokumen23 halamanTreatment Protocol of Snake Bite: Kaushik.H.M 080201388tiruchanurBelum ada peringkat
- Management of Hypertensive EmergencyDokumen35 halamanManagement of Hypertensive EmergencyRaditya Indah TofaniBelum ada peringkat
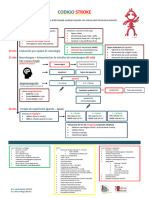
- Codigo Stroke 2Dokumen1 halamanCodigo Stroke 2Gabriela RuizBelum ada peringkat
- Pemicu 6 KGD DeniseDokumen95 halamanPemicu 6 KGD DeniseVincent VandestyoBelum ada peringkat
- STEMI NotesDokumen8 halamanSTEMI NotesIzzul HafiyBelum ada peringkat
- Acute Myocardial Infarction: Recognition and AssessmentDokumen7 halamanAcute Myocardial Infarction: Recognition and AssessmentHasnainKhimjiBelum ada peringkat
- Critical Care Drugs OverviewDokumen23 halamanCritical Care Drugs OverviewAsri Ernadi100% (1)
- Anticoagulation Protocol For PostDokumen8 halamanAnticoagulation Protocol For PostMohammed IbrahimBelum ada peringkat
- Slus 004.85Dokumen1 halamanSlus 004.85Surya AtmajaBelum ada peringkat
- Wartegg Test PDFDokumen1 halamanWartegg Test PDFSurya AtmajaBelum ada peringkat
- DX Management Cellulitis B MJ 1208Dokumen4 halamanDX Management Cellulitis B MJ 1208Surya AtmajaBelum ada peringkat
- Changing Ethics and The Hippocrates Oath ORTOJ 2 E003Dokumen5 halamanChanging Ethics and The Hippocrates Oath ORTOJ 2 E003Surya AtmajaBelum ada peringkat
- Invasive Neuromonitoring TechniqueDokumen20 halamanInvasive Neuromonitoring TechniqueReza ManefoBelum ada peringkat
- Stage 2 PDHPE Scope and SequenceDokumen4 halamanStage 2 PDHPE Scope and SequenceAnthony Dunn100% (1)
- LPL - PSC Ashok Vihar H-62, Lig Flats, Phase-1, Ashok Vihar 9555828281 DelhiDokumen1 halamanLPL - PSC Ashok Vihar H-62, Lig Flats, Phase-1, Ashok Vihar 9555828281 DelhiRahul GuptaBelum ada peringkat
- Upgrading BillsDokumen16 halamanUpgrading BillsMarch BulalacaoBelum ada peringkat
- 74 Poy Casestudy 11 1 PDFDokumen8 halaman74 Poy Casestudy 11 1 PDFDani AzcuetaBelum ada peringkat
- Managing dental patients with cardiovascular diseasesDokumen54 halamanManaging dental patients with cardiovascular diseasesSafiraMaulidaBelum ada peringkat
- Risk Assessment - AbbDokumen3 halamanRisk Assessment - AbbAbdul RaheemBelum ada peringkat
- Kendhujhar Revised MSPLDokumen58 halamanKendhujhar Revised MSPLRakesh MitraBelum ada peringkat
- BJSTR MS Id 004577Dokumen8 halamanBJSTR MS Id 004577SartajHussainBelum ada peringkat
- Kickball ActivityDokumen2 halamanKickball Activityapi-568501343Belum ada peringkat
- Build Muscle and Strength at HomeDokumen17 halamanBuild Muscle and Strength at HomeMuhammad RamaBelum ada peringkat
- Case Study PresentationDokumen35 halamanCase Study PresentationblairBelum ada peringkat
- Office of The Secretary: Administrative Order (014-ADokumen1 halamanOffice of The Secretary: Administrative Order (014-ACharlemagne Sabio GalamgamBelum ada peringkat
- L5 Children With Emotional or Behavioral DisorderDokumen24 halamanL5 Children With Emotional or Behavioral DisorderAGLDBelum ada peringkat
- Oropharyngeal and Nasopharyngeal Suctioning SkillDokumen3 halamanOropharyngeal and Nasopharyngeal Suctioning SkillCherry Rose Arce SamsonBelum ada peringkat
- Country Partnership Strategy: September 2020Dokumen29 halamanCountry Partnership Strategy: September 2020hibonardoBelum ada peringkat
- Scar Endometriosis Case Report With Literature ReviewDokumen3 halamanScar Endometriosis Case Report With Literature ReviewelsaBelum ada peringkat
- Inverted Uterus GuidelinesDokumen2 halamanInverted Uterus GuidelinesEndang Sri WidiyantiBelum ada peringkat
- Music Therapy PsychiatryDokumen59 halamanMusic Therapy PsychiatryAlberto ChicaybanBelum ada peringkat
- Scope of Human RightsDokumen14 halamanScope of Human RightsJohn Lester Tan100% (2)
- Chapter 1Dokumen9 halamanChapter 1atazanjearickBelum ada peringkat
- Material Safety Data Sheet: 1. Company and Product IdentificationDokumen8 halamanMaterial Safety Data Sheet: 1. Company and Product IdentificationYan MoraesBelum ada peringkat
- Drug EducationDokumen5 halamanDrug EducationChristina Lafayette SesconBelum ada peringkat
- Adhd Mary SalantoDokumen58 halamanAdhd Mary SalantoayzlimBelum ada peringkat
- Office Based DLCO Tests Help Pulmonologists To Make Important Clinical DecisionsDokumen7 halamanOffice Based DLCO Tests Help Pulmonologists To Make Important Clinical DecisionstiarapolarisiriuzBelum ada peringkat
- USPH Child Activity ChecklistDokumen1 halamanUSPH Child Activity ChecklistJelena Radonjic CavorBelum ada peringkat
- Diary POC and TMC - ScribdDokumen3 halamanDiary POC and TMC - ScribdrapingcocoBelum ada peringkat
- The Mental Health Act, 1987Dokumen52 halamanThe Mental Health Act, 1987Vizohulie Edward WhuorieBelum ada peringkat
- Nclex RN Cram SheetDokumen7 halamanNclex RN Cram Sheetalsdkfj100% (2)
- Lung Cancer Pathology and DiagnosisDokumen28 halamanLung Cancer Pathology and DiagnosismadvincyBelum ada peringkat