Anda mungkin juga menyukai
- Case Report For Case Presentations Short Rib Polydactyly SyndromeDokumen8 halamanCase Report For Case Presentations Short Rib Polydactyly Syndromeapi-390240132Belum ada peringkat
- Upper Extremity Arterial Protocol 14 PDFDokumen2 halamanUpper Extremity Arterial Protocol 14 PDFapi-390240132Belum ada peringkat
- Case Presentation - Thanatophoric DysplasiaDokumen20 halamanCase Presentation - Thanatophoric Dysplasiaapi-390240132Belum ada peringkat
- Adult Echocardiography Protocol 14 PDFDokumen9 halamanAdult Echocardiography Protocol 14 PDFapi-390240132Belum ada peringkat
- Renal Doppler Protocol 14 PDFDokumen3 halamanRenal Doppler Protocol 14 PDFapi-390240132Belum ada peringkat
- Carotid Protocol 14 PDFDokumen3 halamanCarotid Protocol 14 PDFapi-390240132Belum ada peringkat
- Lower Extremity Arterial Protocol 14 PDFDokumen2 halamanLower Extremity Arterial Protocol 14 PDFapi-390240132Belum ada peringkat
- Ob Biophysical Profile Protocol r14 PDFDokumen3 halamanOb Biophysical Profile Protocol r14 PDFapi-390240132Belum ada peringkat
- Liver Protocol 14 PDFDokumen4 halamanLiver Protocol 14 PDFapi-390240132Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Facomatosis Pubmed PDFDokumen8 halamanFacomatosis Pubmed PDFKevin ChaucaBelum ada peringkat
- Introduction To Heart Tube FormationDokumen33 halamanIntroduction To Heart Tube FormationAarushi JainBelum ada peringkat
- Chapter 10 KSSM FORM 4 BIODokumen12 halamanChapter 10 KSSM FORM 4 BIOYEO MING HUI MoeBelum ada peringkat
- DPP XI Chapter - 18 Body Fluids and Circulation 22Dokumen23 halamanDPP XI Chapter - 18 Body Fluids and Circulation 22Riya MondalBelum ada peringkat
- Q2 W1 D1 English 6Dokumen25 halamanQ2 W1 D1 English 6Nestor MadiBelum ada peringkat
- Pig Heart DissectionDokumen7 halamanPig Heart DissectionJannah Renee TANGONBelum ada peringkat
- Heartbeat Sequencing Colour by NumbersDokumen5 halamanHeartbeat Sequencing Colour by NumbersKavs KitchensBelum ada peringkat
- Physiology of Respiration - Mechanism of Respiration, GaseousDokumen39 halamanPhysiology of Respiration - Mechanism of Respiration, GaseousRakesh KumarBelum ada peringkat
- Pregnancy ManualDokumen73 halamanPregnancy ManualDenisa Myrta100% (2)
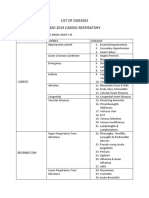
- List of Diseases Imo 2019 Cardio-RespiratoryDokumen2 halamanList of Diseases Imo 2019 Cardio-RespiratoryDimas Adjie Yuda MahendraBelum ada peringkat
- Science Class 8 Respiration and CirculationDokumen9 halamanScience Class 8 Respiration and Circulationamnakazmi100% (1)
- Will This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Dokumen12 halamanWill This Hemodynamically Unstable Patient Respond To A Bolus of Intravenous Fluids?Roberto López MataBelum ada peringkat
- Zoology Finals ReviewerDokumen18 halamanZoology Finals ReviewerZian Lei MienBelum ada peringkat
- Complications of PuerperiumDokumen45 halamanComplications of PuerperiumsubashikBelum ada peringkat
- Book The Luo VesselsDokumen66 halamanBook The Luo VesselsNilton100% (3)
- Blood Vessels and Circulation 1Dokumen36 halamanBlood Vessels and Circulation 1Kuya RnJBelum ada peringkat
- 1st Quarter Exam - ScienceDokumen4 halaman1st Quarter Exam - ScienceMeljean Kalaw Castillo100% (1)
- Frog PPTDokumen30 halamanFrog PPTJundyGumaBelum ada peringkat
- Peripheral Edema: ReviewDokumen7 halamanPeripheral Edema: ReviewVmsdBelum ada peringkat
- Autopsy: Forensic Medicine & Toxicology, NMCDokumen106 halamanAutopsy: Forensic Medicine & Toxicology, NMCAiman sadiq shahBelum ada peringkat
- Scheme of Work Grade 9 2023Dokumen2 halamanScheme of Work Grade 9 2023ramloghun veerBelum ada peringkat
- Management of Monochorionic Twin PregnancyDokumen2 halamanManagement of Monochorionic Twin PregnancyWira PutriBelum ada peringkat
- (Template) DVTDokumen21 halaman(Template) DVTPema Lamu TdkBelum ada peringkat
- Cardiovascular System-GlosaryDokumen3 halamanCardiovascular System-GlosaryJennevi BrunoBelum ada peringkat
- Transport in HumansDokumen6 halamanTransport in HumansSadiaBelum ada peringkat
- Transport System in HumanDokumen7 halamanTransport System in HumanMSMohanaBelum ada peringkat
- Exploring Anatomy Circulatory System WorksheetDokumen4 halamanExploring Anatomy Circulatory System WorksheetBrian MartinezBelum ada peringkat
- Anatomy and Physiology of HeartDokumen5 halamanAnatomy and Physiology of HeartAmit MartinBelum ada peringkat
- Breath by Harold W Percival PDFDokumen4 halamanBreath by Harold W Percival PDFalberttades5883Belum ada peringkat
- Anatomy CoronaryDokumen6 halamanAnatomy Coronarybri bugelBelum ada peringkat