Anda mungkin juga menyukai
- Skeletal System Parts and FunctionsDokumen16 halamanSkeletal System Parts and FunctionsKathleenJoyGalAlmasinBelum ada peringkat
- Human Skeletal SystemDokumen5 halamanHuman Skeletal SystemDrexel DalaygonBelum ada peringkat
- Skeletal System: The CraniumDokumen7 halamanSkeletal System: The CraniumMohamed MustafeBelum ada peringkat
- The Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Dokumen17 halamanThe Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Leo Cordel Jr.Belum ada peringkat
- SKELETALSYSTEMDokumen14 halamanSKELETALSYSTEMvaleree heart abejuelaBelum ada peringkat
- What is the Skeletal SystemDokumen2 halamanWhat is the Skeletal SystemJared RodriguezBelum ada peringkat
- Skeletal SystemDokumen7 halamanSkeletal SystemJovi Floresca AberinBelum ada peringkat
- Skeletal and Integumentary SystemDokumen20 halamanSkeletal and Integumentary SystemAbby Gaile LopezBelum ada peringkat
- Lab Report Skeletal SystemDokumen9 halamanLab Report Skeletal SystemLiza Shi0% (1)
- Introduction To Human Skeletal SystemDokumen12 halamanIntroduction To Human Skeletal SystemKristine DomacenaBelum ada peringkat
- Laboratory 3 SkeletalDokumen9 halamanLaboratory 3 SkeletalKyla InoferioBelum ada peringkat
- The Skeletal System Provides Shape and SupportDokumen2 halamanThe Skeletal System Provides Shape and SupportGrace Ann MeronBelum ada peringkat
- Bones and Muscle 1Dokumen4 halamanBones and Muscle 1Luciely Castro YatesBelum ada peringkat
- Skripta Za Usmeni Iz EngleskogDokumen15 halamanSkripta Za Usmeni Iz EngleskogElizabetaBelum ada peringkat
- PDS01A- Lesson 1Dokumen30 halamanPDS01A- Lesson 1aresfenrirBelum ada peringkat
- The Skeletal SystemDokumen10 halamanThe Skeletal SystemJessa Mae BanquirigBelum ada peringkat
- BONEDokumen27 halamanBONEVIJAYA KUMAR YBelum ada peringkat
- Skeletal System LessonDokumen3 halamanSkeletal System LessonLiwayway De AsisBelum ada peringkat
- Osteocytes - Bone Cells Classifications of Bones According To SizeDokumen17 halamanOsteocytes - Bone Cells Classifications of Bones According To SizeA CBelum ada peringkat
- Cat Quiz Ana AnsDokumen4 halamanCat Quiz Ana AnsDaniel WachiraBelum ada peringkat
- Skeletal System 1Dokumen31 halamanSkeletal System 1Hannan AliBelum ada peringkat
- Skeletal System AnatomyDokumen6 halamanSkeletal System AnatomymanuelaristotleBelum ada peringkat
- The Skeletal System: Bones, Structure and FunctionsDokumen29 halamanThe Skeletal System: Bones, Structure and FunctionsReynaBaquillerBelum ada peringkat
- DefinitionDokumen8 halamanDefinitionJamesBelum ada peringkat
- Musculoskeletal System For BMDokumen13 halamanMusculoskeletal System For BMNepimuga OliverBelum ada peringkat
- Skeletal System Anatomy and Functions in 38 CharactersDokumen5 halamanSkeletal System Anatomy and Functions in 38 CharactersMichael Villamor100% (1)
- Primary Sources of the Skeletal SystemDokumen8 halamanPrimary Sources of the Skeletal SystemJules ConcepcionBelum ada peringkat
- Skeletal System Anatomy GuideDokumen3 halamanSkeletal System Anatomy GuideCk DhiyanBelum ada peringkat
- Modul Anatomi: Fakultas Kedokteran Universitas Islam Malang 2018Dokumen11 halamanModul Anatomi: Fakultas Kedokteran Universitas Islam Malang 2018yournightBelum ada peringkat
- The Musculoskeletal SystemDokumen7 halamanThe Musculoskeletal SystemxoxogeloBelum ada peringkat
- Axial Skeleton Second LectureDokumen23 halamanAxial Skeleton Second LectureRichard BidalBelum ada peringkat
- Pertemuan Ke 7Dokumen3 halamanPertemuan Ke 7Sukma WulandariBelum ada peringkat
- Anaphy ReportingDokumen17 halamanAnaphy ReportingKIA KHYTE FLORESBelum ada peringkat
- Axial Skeleton ScriptDokumen4 halamanAxial Skeleton ScriptMichaelVincentLimBelum ada peringkat
- Skeletal SystemDokumen62 halamanSkeletal SystemAlyza AlcazarinBelum ada peringkat
- Anatomy Notes For BS: Khyber Medical University Peshawar Prepared by DR, Raheel Ahmad Lecturer Pihms. PeshawarDokumen84 halamanAnatomy Notes For BS: Khyber Medical University Peshawar Prepared by DR, Raheel Ahmad Lecturer Pihms. PeshawarShimmering MoonBelum ada peringkat
- Musculoskeletal SystemDokumen17 halamanMusculoskeletal SystemSudhanshu PandeyBelum ada peringkat
- ANAT 100 - Module 2 Summary NotesDokumen6 halamanANAT 100 - Module 2 Summary NotesRahul BhardwajBelum ada peringkat
- Skeletal and Facial Bone AnatomyDokumen12 halamanSkeletal and Facial Bone AnatomyAubrey Unique Evangelista100% (2)
- Appendicular SkeletonDokumen6 halamanAppendicular SkeletonJohn Snow1Belum ada peringkat
- Human Anatomy 4th Edition Saladin Solutions Manual DownloadDokumen9 halamanHuman Anatomy 4th Edition Saladin Solutions Manual DownloadArturo Thomas100% (29)
- ANATOMY I Lecture 02, GENERAL ANATOMY 2, Skeletal System, BonesDokumen42 halamanANATOMY I Lecture 02, GENERAL ANATOMY 2, Skeletal System, BonesHalima NazarBelum ada peringkat
- Skeletal SystemDokumen17 halamanSkeletal SystemDEVBelum ada peringkat
- The Axial Skeleton:: The Skeleton of The Head (Skull) and Trunk (Ribs)Dokumen19 halamanThe Axial Skeleton:: The Skeleton of The Head (Skull) and Trunk (Ribs)Bryan BatallerBelum ada peringkat
- Upper and Lower EkstremityDokumen4 halamanUpper and Lower EkstremitySusantimarilalanBelum ada peringkat
- ACT 5 - Skeletal - Lab Sheet 2 Copy KoDokumen12 halamanACT 5 - Skeletal - Lab Sheet 2 Copy KoMariah Ray RintBelum ada peringkat
- Anatomy and Physiology of the Skeletal SystemDokumen13 halamanAnatomy and Physiology of the Skeletal SystemJo BesandeBelum ada peringkat
- The Skeletal System: Bones, Joints and Functions in 40 CharactersDokumen61 halamanThe Skeletal System: Bones, Joints and Functions in 40 Charactersdrin zekaBelum ada peringkat
- Anatomy and PhysiologyDokumen19 halamanAnatomy and PhysiologyJo BesandeBelum ada peringkat
- Suffixes: Forget, Use - Ful Forgetful, UsefulDokumen5 halamanSuffixes: Forget, Use - Ful Forgetful, UsefulKiks NoyaBelum ada peringkat
- Nursing AnaPhy-Skeletal System Axial SkeletonDokumen29 halamanNursing AnaPhy-Skeletal System Axial SkeletonGail Chantel Spring PerlasBelum ada peringkat
- Skeletal System 5 Functions of The Skeletal SystemDokumen4 halamanSkeletal System 5 Functions of The Skeletal SystemShaira CogollodoBelum ada peringkat
- A Basic UnderstandingDokumen6 halamanA Basic Understandingjessica160793Belum ada peringkat
- The Skeletal SystemDokumen7 halamanThe Skeletal SystemBea GualbertoBelum ada peringkat
- The Human Skeleton: DifferentDokumen5 halamanThe Human Skeleton: DifferentChae Mie Hnin EainBelum ada peringkat
- SkeletalsystemDokumen43 halamanSkeletalsystemSamantha EllaineBelum ada peringkat
- Education Notes 5Dokumen5 halamanEducation Notes 5Rwynn MemoryBelum ada peringkat
- The Skeleton Chapter 7Dokumen6 halamanThe Skeleton Chapter 7rheamii18Belum ada peringkat
- Anes Airway-IntubationDokumen12 halamanAnes Airway-IntubationSGD5Christine MendozaBelum ada peringkat
- Amoebiasis Case PresentationDokumen28 halamanAmoebiasis Case Presentationjan micah100% (1)
- Vomiting Dog Yellow - Google SearchDokumen1 halamanVomiting Dog Yellow - Google SearchCLIFFORD JUANBelum ada peringkat
- Exercise 11 Activity 1Dokumen4 halamanExercise 11 Activity 1MEGAN NICOLE PERNILLA HERNANDEZBelum ada peringkat
- Cell Fractionation & Marker EnzymesDokumen20 halamanCell Fractionation & Marker EnzymesVivek PBelum ada peringkat
- Medical Physiology Membrane PotentialsDokumen39 halamanMedical Physiology Membrane PotentialssanggetharBelum ada peringkat
- Facial Soft-Tissue Spaces and Retaining Ligaments of The Midcheek - Defining The Premaxillary SpaceDokumen8 halamanFacial Soft-Tissue Spaces and Retaining Ligaments of The Midcheek - Defining The Premaxillary SpaceDaniel CoelhoBelum ada peringkat
- Duke University - Medical Neuroscience - by Leonard E. White, Ph.D.Dokumen16 halamanDuke University - Medical Neuroscience - by Leonard E. White, Ph.D.Ejogheneta OnojakeBelum ada peringkat
- Chapter 7 Lab Assignment - Axial Skeleton BonesDokumen5 halamanChapter 7 Lab Assignment - Axial Skeleton Bonesadriana blanco galianoBelum ada peringkat
- Plant and Animal Organs Systems P1Dokumen8 halamanPlant and Animal Organs Systems P1ian laurence pedranoBelum ada peringkat
- Leson Plan FEMALE PELVISDokumen8 halamanLeson Plan FEMALE PELVISPreeti SawantBelum ada peringkat
- Laryngeal Anatomy and Airway ManagementDokumen15 halamanLaryngeal Anatomy and Airway ManagementMeahgan Renee FeudoBelum ada peringkat
- Autoimmune Disease MechanismsDokumen6 halamanAutoimmune Disease MechanismsHaliunaa BattulgaBelum ada peringkat
- Anaphy ReviewerDokumen19 halamanAnaphy ReviewerGian Paolo P. CHAVEZBelum ada peringkat
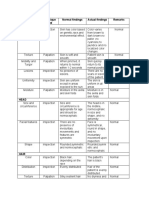
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDokumen6 halamanArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosBelum ada peringkat
- Case Study (Bronchial Asthma)Dokumen11 halamanCase Study (Bronchial Asthma)DhanNie Cenita50% (2)
- Cancer Cytopathology - 2017 - La Fortune - Improvements in Cell Block Processing The Cell Gel MethodDokumen10 halamanCancer Cytopathology - 2017 - La Fortune - Improvements in Cell Block Processing The Cell Gel MethodVlad TomaBelum ada peringkat
- Antiphospholipid Syndrome: Causes, Diagnosis and Treatment of Pregnancy ComplicationsDokumen26 halamanAntiphospholipid Syndrome: Causes, Diagnosis and Treatment of Pregnancy ComplicationsDyn AdrianiBelum ada peringkat
- XIYAN (MN-LE-16) : Eyes of The KneeDokumen1 halamanXIYAN (MN-LE-16) : Eyes of The Kneeray72roBelum ada peringkat
- Parts of a Cow ExplainedDokumen1 halamanParts of a Cow Explainedalfonzo baquedanoBelum ada peringkat
- Exercise Chapter 12Dokumen10 halamanExercise Chapter 12Nurul HusnaBelum ada peringkat
- Year 4 Reading Your Digestive SystemDokumen11 halamanYear 4 Reading Your Digestive SystemMa Donabel LopezBelum ada peringkat
- Brain Review JeopardyDokumen51 halamanBrain Review Jeopardyapi-261267976Belum ada peringkat
- Female Reproductive AnatomydDokumen7 halamanFemale Reproductive AnatomydOneda Ganbatte' KudasaiBelum ada peringkat
- Ilovepdf MergedDokumen457 halamanIlovepdf MergedMar LoyolaBelum ada peringkat
- Making Up For Lost TimeDokumen8 halamanMaking Up For Lost TimemochimochiBelum ada peringkat
- Science 6 2ND QuarterDokumen1 halamanScience 6 2ND QuarterPSALMS KEILAH BANTOGBelum ada peringkat
- Ayesha MuzaffarDokumen31 halamanAyesha MuzaffarpashaBelum ada peringkat
- VahimetsmartinDokumen0 halamanVahimetsmartinAngela PagliusoBelum ada peringkat
- Prelim HPCTDokumen37 halamanPrelim HPCTMariaangela AliscuanoBelum ada peringkat