Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- RStudio ExercicesDokumen8 halamanRStudio ExercicesVania BatistaBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Dosimetric Consequences of Pencil Beam Width Variations in Scanned Beam Particle TherapyDokumen16 halamanDosimetric Consequences of Pencil Beam Width Variations in Scanned Beam Particle TherapyVania BatistaBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- AAPM Proton Therapy PDFDokumen85 halamanAAPM Proton Therapy PDFVania Batista100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Booklet n3 Physics For ClinrtDokumen166 halamanBooklet n3 Physics For Clinrtjts99athotmaildotcomBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Demons AlgorithmDokumen12 halamanThe Demons AlgorithmVania BatistaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- AAPM Task 43Dokumen29 halamanAAPM Task 43Vania BatistaBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Ultrasonic Diffraction in LiquidsDokumen5 halamanUltrasonic Diffraction in LiquidsSampriti ShomeBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Beryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimDokumen28 halamanBeryllium and Beryllium Compounds: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimjaimeBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Submodular Set Function - WikipediaDokumen5 halamanSubmodular Set Function - WikipedianmahsevBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Adjoint Rans With Filtered Shape Derivatives For Hydrodynamic OptimisationDokumen11 halamanAdjoint Rans With Filtered Shape Derivatives For Hydrodynamic Optimisationvolo87Belum ada peringkat
- RCE2018 math and geometry problems solutions under 40 charactersDokumen1 halamanRCE2018 math and geometry problems solutions under 40 charactersArwin VillegasBelum ada peringkat
- Assignment 1Dokumen3 halamanAssignment 1V V Swarat Sasa50% (2)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Principles of CT and CT TechnologyDokumen15 halamanPrinciples of CT and CT TechnologyLida Velasquez SierraBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Galloway 1989 Genetic Stratigraphic Sequence Basin Analysis IDokumen18 halamanGalloway 1989 Genetic Stratigraphic Sequence Basin Analysis IMitreBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Heat Exchangers Types & Applications, LMTD Derivation & ProblemsDokumen11 halamanHeat Exchangers Types & Applications, LMTD Derivation & Problemsananth2012Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- 4363 111 Machine Design IDokumen6 halaman4363 111 Machine Design Iyogesh_b_k100% (2)
- How To Build With CobDokumen33 halamanHow To Build With CobmandritsopoulosBelum ada peringkat
- Zetex HandbookDokumen8 halamanZetex HandbookbolermBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- GannZilla User GuideDokumen20 halamanGannZilla User GuideNiladri Jana100% (26)
- ZDokumen265 halamanZAdal ContrerasBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Soal Bahasa InggrisDokumen7 halamanSoal Bahasa InggrisPelkeh Prianda25% (16)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Maxwell Stress Tensor ExplainedDokumen6 halamanMaxwell Stress Tensor ExplainedSyeda Tehreem IqbalBelum ada peringkat
- BS 476.6 PDFDokumen10 halamanBS 476.6 PDFJmc NarelaBelum ada peringkat
- ENGGPHYSDokumen13 halamanENGGPHYSUploader101Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Elzaki Transform For Two Tank Mixing Problems PDFDokumen15 halamanElzaki Transform For Two Tank Mixing Problems PDFMarvin LabajoBelum ada peringkat
- CH 10 Circular Motion Exercises AnswersDokumen4 halamanCH 10 Circular Motion Exercises AnswersMuhammad Aslam0% (1)
- Interactions and Incompatibilities of Pharmaceutical ExcipientsDokumen24 halamanInteractions and Incompatibilities of Pharmaceutical ExcipientsEmmanuel Vachon LachanceBelum ada peringkat
- Force & FrictionDokumen9 halamanForce & Frictionbinu_praveen100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Motion Programming For ComauDokumen318 halamanMotion Programming For ComauEddie Scarpa100% (1)
- MCQ Electromagnetism Self-AssessmentDokumen2 halamanMCQ Electromagnetism Self-AssessmentJunaidKhanBelum ada peringkat
- Mean Deviation - Wolfram MathWorldDokumen4 halamanMean Deviation - Wolfram MathWorldbraulio.dantas-1Belum ada peringkat
- Harmonic Oscillator & Rigid Rotor ModelsDokumen14 halamanHarmonic Oscillator & Rigid Rotor ModelsJisu RyuBelum ada peringkat
- Jawaharlal Nehru Technological University KakinadaDokumen4 halamanJawaharlal Nehru Technological University KakinadaVenkat ChadalavadaBelum ada peringkat
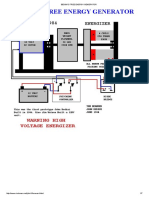
- Bedini's Free Energy Generator PDFDokumen7 halamanBedini's Free Energy Generator PDFRafly Attila Al-Fiqri71% (7)
- Physics Questions Part 3Dokumen8 halamanPhysics Questions Part 3Muhammad HuzaifaBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)