Anda mungkin juga menyukai
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionDari EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionBelum ada peringkat
- 76) Book Chapter 2010Dokumen11 halaman76) Book Chapter 2010Giovanni MauroBelum ada peringkat
- Perspective: Placebo Effects: From The Neurobiological Paradigm To Translational ImplicationsDokumen2 halamanPerspective: Placebo Effects: From The Neurobiological Paradigm To Translational ImplicationsALEXIS ANDRES HUAYLLA DE LA CRUZBelum ada peringkat
- Mechanisms Involved in Placebo and Nocebo Responses and Implications For Drug TrialsDokumen5 halamanMechanisms Involved in Placebo and Nocebo Responses and Implications For Drug TrialsAlfredo GarciaBelum ada peringkat
- 2017 - Mar - The Placebo and Nocebo Phenomena. Their Clinical Management and Impact On Treatment Outcomes (Read - MB)Dokumen10 halaman2017 - Mar - The Placebo and Nocebo Phenomena. Their Clinical Management and Impact On Treatment Outcomes (Read - MB)brumontoroBelum ada peringkat
- Neurobiological Mechanism of The Placebo EffectDokumen13 halamanNeurobiological Mechanism of The Placebo EffectAna-Maria BadescuBelum ada peringkat
- Studies On The Mechanism and Impacts of Placebo Effect Illness and Interpersonal HealingDokumen5 halamanStudies On The Mechanism and Impacts of Placebo Effect Illness and Interpersonal HealingInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Benedetti 2006Dokumen3 halamanBenedetti 2006Alejandra CachoBelum ada peringkat
- A Review of The Theoretical and Biological Understanding of The Nocebo and Placebo PhenomenaDokumen8 halamanA Review of The Theoretical and Biological Understanding of The Nocebo and Placebo PhenomenaRealidades InfinitasBelum ada peringkat
- Placebo EffectDokumen22 halamanPlacebo EffectZendaya Slim TargaryenBelum ada peringkat
- Placebo Effect: Shreyasi Pawar, 503Dokumen19 halamanPlacebo Effect: Shreyasi Pawar, 503Shreyasi AnkushBelum ada peringkat
- Oronowicz-Jaśkowiak 2019 PDFDokumen8 halamanOronowicz-Jaśkowiak 2019 PDFJulio JuarezBelum ada peringkat
- Psicologia DolorDokumen8 halamanPsicologia DolorMarlyGabrielaSosaRojasBelum ada peringkat
- Analgesic Effect of Placebo in Clinical Trials: TopicDokumen15 halamanAnalgesic Effect of Placebo in Clinical Trials: TopicPriyanka DeyBelum ada peringkat
- Exposición FinalDokumen4 halamanExposición FinalEmily A Espinoza ArtolaBelum ada peringkat
- The Ethics of The Placebo in Clinical PracticeDokumen5 halamanThe Ethics of The Placebo in Clinical PracticeLam Sin WingBelum ada peringkat
- Efecto Placebo MecanismosDokumen21 halamanEfecto Placebo MecanismosiamidaBelum ada peringkat
- Vachon-Presseau 2018Dokumen15 halamanVachon-Presseau 2018RashidkpvldBelum ada peringkat
- Placebo Effects in MedicineDokumen11 halamanPlacebo Effects in MedicineTaufik Ghockil ZlaluwBelum ada peringkat
- Medicine's Inconvenient Truth: The Placebo and Nocebo EffectDokumen8 halamanMedicine's Inconvenient Truth: The Placebo and Nocebo EffectNestor AndresBelum ada peringkat
- Placebo Neurofeedback PDFDokumen13 halamanPlacebo Neurofeedback PDFJulianaTeixeiraBelum ada peringkat
- Placebo Article in ArchivesDokumen12 halamanPlacebo Article in ArchivesIsak Isakov100% (2)
- Snomed CT RL (Outline)Dokumen23 halamanSnomed CT RL (Outline)kostya111Belum ada peringkat
- Neurexan - The Bioregulatory Approach To The Treatment of Stress (Bases Preclinicas y Clinicas Del Estres)Dokumen9 halamanNeurexan - The Bioregulatory Approach To The Treatment of Stress (Bases Preclinicas y Clinicas Del Estres)Cristobal CarrascoBelum ada peringkat
- The Ethics of PlacebosDokumen3 halamanThe Ethics of PlacebosKomisi Skill PMK FK-FKG UHBelum ada peringkat
- How Placebos Change The Patient's BrainDokumen1 halamanHow Placebos Change The Patient's BrainDiana VBelum ada peringkat
- The Effect of Placebo Administration On The First-Night Effect in Healthy Young VolunteersDokumen9 halamanThe Effect of Placebo Administration On The First-Night Effect in Healthy Young VolunteersbtchcamebackBelum ada peringkat
- How Do Placebos WorkDokumen3 halamanHow Do Placebos Workapi-443830029Belum ada peringkat
- Placebo Effect: The Power of BeliefDokumen3 halamanPlacebo Effect: The Power of BeliefoehebakBelum ada peringkat
- Early Discontinuation of ASM in Neonatal Seizure - CommentDokumen5 halamanEarly Discontinuation of ASM in Neonatal Seizure - CommentMariela Nadir Guerreros De VelasquezBelum ada peringkat
- The Placebo EffectDokumen7 halamanThe Placebo Effectapi-583543995Belum ada peringkat
- Fpsyt 14 1301143Dokumen8 halamanFpsyt 14 1301143nakomang513Belum ada peringkat
- Placebo TheoryDokumen23 halamanPlacebo Theoryiron9962Belum ada peringkat
- Collins y Pinch-Dr. Golem Cap. 1Dokumen17 halamanCollins y Pinch-Dr. Golem Cap. 1andrecast303Belum ada peringkat
- Hypothesis: Placebo Analgesia, Acupuncture and Sham SurgeryDokumen6 halamanHypothesis: Placebo Analgesia, Acupuncture and Sham SurgeryHeHICBelum ada peringkat
- Efecto Placebo2Dokumen6 halamanEfecto Placebo2Marja GuízarBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen20 halamanNIH Public Access: Author ManuscriptRamarao CHBelum ada peringkat
- tmp33F4 TMPDokumen7 halamantmp33F4 TMPFrontiersBelum ada peringkat
- Neurology 2017 Feigin 2160 1Dokumen3 halamanNeurology 2017 Feigin 2160 1royBelum ada peringkat
- The Effect of General Anesthesia On Neurocognitive Development in Early ChildhoodDokumen23 halamanThe Effect of General Anesthesia On Neurocognitive Development in Early ChildhoodRin4lBelum ada peringkat
- Class GrecochibchaDokumen9 halamanClass GrecochibchaPablo A.Belum ada peringkat
- Placebo Effect Thesis StatementDokumen7 halamanPlacebo Effect Thesis StatementChristine Williams100% (2)
- Place BooDokumen3 halamanPlace BooYosepha HutaurukBelum ada peringkat
- Thesis Statement Placebo EffectDokumen5 halamanThesis Statement Placebo Effectamberbutlervirginiabeach100% (2)
- Vidal 2011Dokumen13 halamanVidal 2011xoxomeBelum ada peringkat
- Beyond Dopamine Receptor Antagonism, New Targets For SCZ Treatment and PreventionDokumen18 halamanBeyond Dopamine Receptor Antagonism, New Targets For SCZ Treatment and Preventionjanicesusanto2000Belum ada peringkat
- Placebo Effect Literature ReviewDokumen5 halamanPlacebo Effect Literature Reviewukefbfvkg100% (1)
- Placebo FinalDokumen9 halamanPlacebo FinalRica Jane TorresBelum ada peringkat
- The Neurobiological Underpinnings of AddictionDokumen9 halamanThe Neurobiological Underpinnings of AddictionShaun Shelly100% (1)
- WFSBP Consensus Paper Biological Markers in DepressionDokumen34 halamanWFSBP Consensus Paper Biological Markers in Depressionscabrera_scribdBelum ada peringkat
- Nihm Molekular Neurobiologi Deprsi 2007Dokumen10 halamanNihm Molekular Neurobiologi Deprsi 2007srihandayani1984Belum ada peringkat
- Chronic Insomnia: Matt T. Bianchi, MD, PHDDokumen6 halamanChronic Insomnia: Matt T. Bianchi, MD, PHDAlex BorroelBelum ada peringkat
- 69) Jop Paper 2009Dokumen15 halaman69) Jop Paper 2009Giovanni MauroBelum ada peringkat
- Thesis Placebo EffectDokumen8 halamanThesis Placebo Effectbshpab74100% (2)
- KIRMAYER, Laurence. Unpacking The Placebo ResponseDokumen13 halamanKIRMAYER, Laurence. Unpacking The Placebo ResponseManuel Canavarros GirardBelum ada peringkat
- Klinger 2014Dokumen4 halamanKlinger 2014Alejandra CachoBelum ada peringkat
- Sleep DeprivationDokumen25 halamanSleep Deprivationdefaagri50% (4)
- Ni Hms 749680Dokumen32 halamanNi Hms 749680Cristian GhiţăBelum ada peringkat
- Placebo TreatmentDokumen4 halamanPlacebo TreatmentnusmaizaBelum ada peringkat
- Placebo and Non-Specific Effects - KelseyDokumen19 halamanPlacebo and Non-Specific Effects - KelseyVíctor Chaves MuñozBelum ada peringkat
- Voluntary Internship Scheme For Law StudentsDokumen1 halamanVoluntary Internship Scheme For Law StudentsVikhyat NareshBelum ada peringkat
- Nir Sity of Sci Ce and Technology: Ma Univer enDokumen2 halamanNir Sity of Sci Ce and Technology: Ma Univer enVikhyat NareshBelum ada peringkat
- Nirma University of Science and TechnologyDokumen2 halamanNirma University of Science and TechnologyVikhyat NareshBelum ada peringkat
- Nirm Uni R Ity: A Ve S of Science and TechnologyDokumen1 halamanNirm Uni R Ity: A Ve S of Science and TechnologyVikhyat NareshBelum ada peringkat
- Articles Related To Union and Its Territory at A GlanceDokumen27 halamanArticles Related To Union and Its Territory at A GlanceVikhyat NareshBelum ada peringkat
- Effect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsDokumen12 halamanEffect of Toe Treatments On The Fatigue Resistance of Structural Steel WeldsVicente Palazzo De MarinoBelum ada peringkat
- Be Project Presentation SuspensionDokumen17 halamanBe Project Presentation SuspensionGabrielBelum ada peringkat
- 03N - Top Level View of Computer Function and InterconnectionDokumen38 halaman03N - Top Level View of Computer Function and InterconnectionDoc TelBelum ada peringkat
- 11 Physical Fitness Assessment 1Dokumen40 halaman11 Physical Fitness Assessment 1Danilo Sare IIIBelum ada peringkat
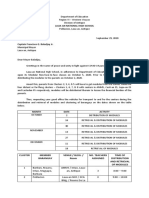
- Module Letter 1Dokumen2 halamanModule Letter 1eeroleBelum ada peringkat
- Hypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Dokumen289 halamanHypochondriasis and Health Anxiety - A Guide For Clinicians (PDFDrive)Fernanda SilvaBelum ada peringkat
- The Heart: Dr. Silvia BoyajianDokumen44 halamanThe Heart: Dr. Silvia BoyajianAsem YousefBelum ada peringkat
- Brochure - Citadines Flatiron Phnom Penh - EnglishDokumen4 halamanBrochure - Citadines Flatiron Phnom Penh - EnglishTix VirakBelum ada peringkat
- 100 Câu Viết Lại Câu Ôn Thi Vào Lóp 6Dokumen10 halaman100 Câu Viết Lại Câu Ôn Thi Vào Lóp 6Nguyễn Thanh PhươngBelum ada peringkat
- Prerak BhavsarDokumen1 halamanPrerak Bhavsarprerakb456gmailcomBelum ada peringkat
- CON21 6th EditionDokumen65 halamanCON21 6th EditionDavid WeeBelum ada peringkat
- Iso 3932 1976Dokumen8 halamanIso 3932 1976NaveedBelum ada peringkat
- Chapter 5 Pneumatic and Hydraulic Actuation SystemsDokumen22 halamanChapter 5 Pneumatic and Hydraulic Actuation SystemsMukhammad FauzyBelum ada peringkat
- Nelson Tables All in One PDFDokumen618 halamanNelson Tables All in One PDFAmulya Ramakrishna100% (7)
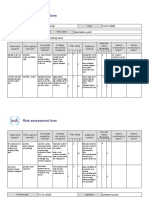
- Risk Assessment Project Iosh - MsDokumen2 halamanRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- Apti 2Dokumen17 halamanApti 2Arunkumar MurugappanBelum ada peringkat
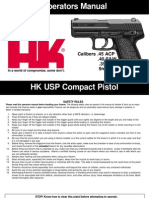
- HK USP CompactDokumen56 halamanHK USP CompactJonathan CrenshawBelum ada peringkat
- DalmatiaDokumen265 halamanDalmatiaomissam2Belum ada peringkat
- PEPSIDokumen99 halamanPEPSIkingloiyaBelum ada peringkat
- Mikrotik Kung Fu Kitab 2Dokumen68 halamanMikrotik Kung Fu Kitab 2aditya ferdiansyahBelum ada peringkat
- ABB Photovoltaic DisconnectorsDokumen6 halamanABB Photovoltaic DisconnectorsBog PenBelum ada peringkat
- Furuno FM 8700 Users Manual 429122Dokumen102 halamanFuruno FM 8700 Users Manual 429122Igor MaranguanheBelum ada peringkat
- Transcendental Meditation (Four Lectures by Silo)Dokumen49 halamanTranscendental Meditation (Four Lectures by Silo)nmjoshi77859100% (2)
- Run Omega Run Lunar Omegaverse Book 5 Shyla Colt All ChapterDokumen52 halamanRun Omega Run Lunar Omegaverse Book 5 Shyla Colt All Chapterkate.brown975100% (6)
- Biology F4 Review Summary NoteDokumen117 halamanBiology F4 Review Summary NoteSocdal AbdiBelum ada peringkat
- DHI-ITALE-060AA-P: White Strobe LampDokumen2 halamanDHI-ITALE-060AA-P: White Strobe LampXlabs MedanBelum ada peringkat
- History of Journalism With Whiteboard StyleDokumen56 halamanHistory of Journalism With Whiteboard StyleXeon JupiterBelum ada peringkat
- Bendable ConcreteDokumen21 halamanBendable ConcreteJulia Sebastian0% (1)
- NSO SPRDokumen9 halamanNSO SPRADITYA SINGHBelum ada peringkat
- Art 16-18Dokumen528 halamanArt 16-18ErudíhenBelum ada peringkat