Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Asetalzolamid 2Dokumen5 halamanAsetalzolamid 2Firstiafina Tiffany100% (1)
- Exercise in Hypobaric, Hyperbaric and Microgravity EnvironmentsDokumen35 halamanExercise in Hypobaric, Hyperbaric and Microgravity EnvironmentsdeepuphysioBelum ada peringkat
- GIO Trekking ManualDokumen43 halamanGIO Trekking ManualGandharva Shankara MurthyBelum ada peringkat
- First Aid of Common Emergencies in Outdoor ActivitiesDokumen9 halamanFirst Aid of Common Emergencies in Outdoor Activitiesrose condezBelum ada peringkat
- PE 4thG QADokumen4 halamanPE 4thG QALiah Mercado100% (1)
- Altitude PDFDokumen47 halamanAltitude PDFMohd AsadBelum ada peringkat
- High Altitude Pulmonary EdemaDokumen5 halamanHigh Altitude Pulmonary EdemaNanda SapitriBelum ada peringkat
- Double Entry Journal - Into Thin AirDokumen5 halamanDouble Entry Journal - Into Thin Airapi-251154045Belum ada peringkat
- World Extreme Medicine Expedition Kit List E BookDokumen11 halamanWorld Extreme Medicine Expedition Kit List E Bookdeejrogers96Belum ada peringkat
- High-Altitude MedicineDokumen12 halamanHigh-Altitude MedicineSBelum ada peringkat
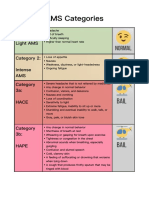
- AMS Categories: Category 1: Light AMS Category 2: Intense AMS Category 3a: HaceDokumen1 halamanAMS Categories: Category 1: Light AMS Category 2: Intense AMS Category 3a: HaceyyggvcBelum ada peringkat
- Common Medical AbbreviationDokumen25 halamanCommon Medical AbbreviationKim Glaidyl BontuyanBelum ada peringkat
- Medication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnessDokumen12 halamanMedication and Dosage Considerations in The Prophylaxis and Treatment of High-Atitude - IllnesslorenzorabbiBelum ada peringkat
- High Altitude Anaesthesia PDFDokumen7 halamanHigh Altitude Anaesthesia PDFK.krishna PriyaBelum ada peringkat
- COMPILATION ON ENVIRONMENTAL DISEASES by Aditi AryaDokumen15 halamanCOMPILATION ON ENVIRONMENTAL DISEASES by Aditi AryaGogi HotiBelum ada peringkat
- Emergency in Respiratory MedicineDokumen73 halamanEmergency in Respiratory MedicineIndra MahaputraBelum ada peringkat
- Corrected Copy Pe 12 Recreational Module 56 2020 2021Dokumen20 halamanCorrected Copy Pe 12 Recreational Module 56 2020 2021Dan Andrei BongoBelum ada peringkat
- Definition of Noncardiogenic Pulmonary Edemanoncardiogenic Pulmonary Edema Is IdentifiedDokumen35 halamanDefinition of Noncardiogenic Pulmonary Edemanoncardiogenic Pulmonary Edema Is IdentifiedAya EyadBelum ada peringkat
- Cardiovascular Adaptation To High-Altitude HypoxiaDokumen19 halamanCardiovascular Adaptation To High-Altitude HypoxiaChethan UpadhyayaBelum ada peringkat
- Homoeopathy For Frost BiteDokumen2 halamanHomoeopathy For Frost BiteDr Dushyant Kamal DhariBelum ada peringkat
- Hipobaric OverviewDokumen9 halamanHipobaric OverviewTrisna AryawanBelum ada peringkat
- Adventure And: Safety Start HereDokumen33 halamanAdventure And: Safety Start HerejltarleyBelum ada peringkat
- Wilderness and Remote First Aid: Emergency Reference GuideDokumen121 halamanWilderness and Remote First Aid: Emergency Reference GuideAdrian Lindemann100% (1)
- Introduction in Hygiene and EcologyDokumen95 halamanIntroduction in Hygiene and EcologyAyad Idres100% (1)
- High Altitude HypoxiaDokumen4 halamanHigh Altitude HypoxiaAbdur Rachman Ba'abdullahBelum ada peringkat
- TRAFFIC JAM in EVERESTDokumen18 halamanTRAFFIC JAM in EVERESTSB100% (1)
- High Altitude Environment Physiology, Adaptations, and IllnessDokumen3 halamanHigh Altitude Environment Physiology, Adaptations, and IllnessJoseph AmeerBelum ada peringkat
- An Anesthesiologist's Guide To Hypoxic Pulmonary Vasoconstriction: Implications For Managing Single-Lung Anesthesia and AtelectasisDokumen10 halamanAn Anesthesiologist's Guide To Hypoxic Pulmonary Vasoconstriction: Implications For Managing Single-Lung Anesthesia and AtelectasisMuchammad FahruludinBelum ada peringkat
- Impact of High Altitude On Cardiovascular Health: Current PerspectivesDokumen19 halamanImpact of High Altitude On Cardiovascular Health: Current PerspectivesveronicaBelum ada peringkat
- Pulmonary Edema II: Noncardiogenic Pulmonary EdemaDokumen31 halamanPulmonary Edema II: Noncardiogenic Pulmonary EdemaGita Helvia SariBelum ada peringkat