Anda mungkin juga menyukai
- 04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseDokumen1 halaman04 02 2021 Engagement Sur L Honneur Plus de 11 Ans Version AnglaiseCarina ColtuneacBelum ada peringkat
- 1990-Fleming Suturing Method and PainDokumen7 halaman1990-Fleming Suturing Method and PainAnonymous bq4KY0mcWG0% (1)
- 1-Adrenocorticosteroids Chapter39Dokumen94 halaman1-Adrenocorticosteroids Chapter39hamidBelum ada peringkat
- CortisolDokumen2 halamanCortisolአብይ በላይነሽ ጥላሁንBelum ada peringkat
- Adrenal Hormones: Pituitary Gland Consists of 3 LobesDokumen9 halamanAdrenal Hormones: Pituitary Gland Consists of 3 LobesMoha MedBelum ada peringkat
- CorticosteroidsDokumen18 halamanCorticosteroidsمحمد العراقيBelum ada peringkat
- Drug StudyDokumen20 halamanDrug Studyvarshasharma05Belum ada peringkat
- Metabolisme KarbohidratDokumen56 halamanMetabolisme KarbohidratAnonymous QCMhA4wNgBBelum ada peringkat
- Assignment of Adrenal CortexDokumen12 halamanAssignment of Adrenal CortexWania AliBelum ada peringkat
- Adrenocorticosteroids & Adrenocortical Antagonists: Namwase Hadijja KatabiraDokumen77 halamanAdrenocorticosteroids & Adrenocortical Antagonists: Namwase Hadijja KatabiraSamson100% (1)
- Adrenocortical HormonesDokumen77 halamanAdrenocortical HormonesMaxamed Faarax XaashiBelum ada peringkat
- Review Glucocorticoids and Fatty Acid Metabolism in Humans: Fuelling Fat Redistribution in The Metabolic SyndromeDokumen16 halamanReview Glucocorticoids and Fatty Acid Metabolism in Humans: Fuelling Fat Redistribution in The Metabolic SyndromeCorona FingerBelum ada peringkat
- 5.2 Principles of Hormonal RegulationsDokumen35 halaman5.2 Principles of Hormonal RegulationsSurvin KandhariBelum ada peringkat
- Adrenal GlandDokumen46 halamanAdrenal GlandhSANBelum ada peringkat
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDokumen34 halamanHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyasBelum ada peringkat
- Basics in Diseases of Adrenal GlandsDokumen7 halamanBasics in Diseases of Adrenal GlandsFrancis ChegeBelum ada peringkat
- Kortizol FizyolojiDokumen5 halamanKortizol FizyolojiVedat KacarBelum ada peringkat
- Sargsyan-Herman2019 Article RegulationOfGlucoseProductionIDokumen11 halamanSargsyan-Herman2019 Article RegulationOfGlucoseProductionIMajo CamargoBelum ada peringkat
- BIOCHEMISTRY ASSIGNMENT HowardDokumen4 halamanBIOCHEMISTRY ASSIGNMENT HowardHoward SakalaBelum ada peringkat
- 6-Adrenocortical Hormones PancreaseDokumen47 halaman6-Adrenocortical Hormones Pancreasetmqt2fbnzgBelum ada peringkat
- Adrenocorticosteroids: Adrenal GlandDokumen51 halamanAdrenocorticosteroids: Adrenal Glandكسلان اكتب اسميBelum ada peringkat
- Hdp301diabetes 2021Dokumen6 halamanHdp301diabetes 2021Linda NguyenBelum ada peringkat
- Diabetic KetoacidosisDokumen16 halamanDiabetic Ketoacidosisjoyshe111100% (2)
- Adrenal Cortex: Functions & Disorders: By: Post Graduate Student Dept. of Oral Medicine, Diagnosis & RadiologyDokumen80 halamanAdrenal Cortex: Functions & Disorders: By: Post Graduate Student Dept. of Oral Medicine, Diagnosis & Radiologyvihang146Belum ada peringkat
- Adrecorticol Hormones and AntagonistsDokumen59 halamanAdrecorticol Hormones and AntagonistsFavourBelum ada peringkat
- GlucocorticoidDokumen10 halamanGlucocorticoidRauf KhanBelum ada peringkat
- Adrenal Glands 2018 - 2019Dokumen32 halamanAdrenal Glands 2018 - 2019Bianca BiaBelum ada peringkat
- Pancreas Aug 4Dokumen53 halamanPancreas Aug 4Dr.Gomathi sivakumarBelum ada peringkat
- Clinical Manifestations: Psammoma BodiesDokumen1 halamanClinical Manifestations: Psammoma BodiesshinaBelum ada peringkat
- Fluid and Electrolyte Therapy in Diabetic KetoacidosisDokumen13 halamanFluid and Electrolyte Therapy in Diabetic KetoacidosisLohJBelum ada peringkat
- SteroidsDokumen22 halamanSteroidsLuqman QadirBelum ada peringkat
- Diabetes Mellitus and Laboratory Tests of DiabetesDokumen24 halamanDiabetes Mellitus and Laboratory Tests of DiabetesturkiBelum ada peringkat
- ADRENAL GLAND X.PPTX - 1Dokumen23 halamanADRENAL GLAND X.PPTX - 1b29jcqnfn9Belum ada peringkat
- Pleg CheckDokumen46 halamanPleg CheckSehrish BajwaBelum ada peringkat
- Metabolism of Adrenal SteroidsDokumen15 halamanMetabolism of Adrenal SteroidsRahmawati RdnBelum ada peringkat
- Carbohydrates PDFDokumen8 halamanCarbohydrates PDFWrigley PatioBelum ada peringkat
- Adrenal GlandDokumen32 halamanAdrenal GlandAlok KumarBelum ada peringkat
- Adrenal DiseasesDokumen66 halamanAdrenal DiseasesNebiyu NegaBelum ada peringkat
- Document 36 (2) .Doc NewDokumen34 halamanDocument 36 (2) .Doc NewPraveen PuthuparambilBelum ada peringkat
- CorticosteroidsDokumen36 halamanCorticosteroidsAbdur RafayBelum ada peringkat
- Endocrine Physiolgy - Lec 04 - Intake 40 - Adrenal GlandDokumen30 halamanEndocrine Physiolgy - Lec 04 - Intake 40 - Adrenal Glanddidulalakshitha39Belum ada peringkat
- Corticosteroids WordDokumen10 halamanCorticosteroids WordMahnoor ArshadBelum ada peringkat
- Glucose MetabolismDokumen48 halamanGlucose MetabolismJay R Plogio100% (1)
- Test 1 - Psio303aDokumen28 halamanTest 1 - Psio303aErika Aranda0% (1)
- 5 - Adrenal Glands (Adrenocorticoids)Dokumen37 halaman5 - Adrenal Glands (Adrenocorticoids)Dr. SaniaBelum ada peringkat
- GluconeogenEZ Control of Blood GlucoseDokumen1 halamanGluconeogenEZ Control of Blood GlucosebirlikteyizBelum ada peringkat
- Corticosteroid: 1 Mineralocorticoids, Mainly Aldosterone in Humans Have SaltretainingDokumen5 halamanCorticosteroid: 1 Mineralocorticoids, Mainly Aldosterone in Humans Have Saltretaining우영박Belum ada peringkat
- 003 - DM - Acute ComplicationsDokumen17 halaman003 - DM - Acute ComplicationsLucas Victor AlmeidaBelum ada peringkat
- Adrenocortical HormonesDokumen5 halamanAdrenocortical HormonesHala RezaBelum ada peringkat
- Hyper MetabolismDokumen4 halamanHyper MetabolismSri AsmawatiBelum ada peringkat
- Alcohol Liver DiseaseDokumen7 halamanAlcohol Liver DiseaseRavi ShankarBelum ada peringkat
- Reg of BGDokumen42 halamanReg of BGSuhayb CumarBelum ada peringkat
- Makerere University: Assay of Glucose by Glucose Oxidase and Glucose Tolerance TestDokumen20 halamanMakerere University: Assay of Glucose by Glucose Oxidase and Glucose Tolerance TestAddiBelum ada peringkat
- Physiology (Compatibility Mode) - 1Dokumen40 halamanPhysiology (Compatibility Mode) - 1ahmad aliBelum ada peringkat
- Pharmacology of Endocrine System-NursingDokumen58 halamanPharmacology of Endocrine System-NursingRaveenmayiBelum ada peringkat
- Introduction To The Endocrine Control On MetabolismDokumen79 halamanIntroduction To The Endocrine Control On Metabolisminka.elseBelum ada peringkat
- Dhupa 1998Dokumen22 halamanDhupa 1998EFRAIN CARDENAS MENDOZABelum ada peringkat
- Age Related Changes in Endocrine SystemDokumen2 halamanAge Related Changes in Endocrine SystemMizrab Nadeem0% (1)
- Signaling Pathways of Glucose in Our Body - PART ONEDokumen9 halamanSignaling Pathways of Glucose in Our Body - PART ONEMaria Jose MartinezBelum ada peringkat
- Glyconeogenesis - BIO 3110Dokumen23 halamanGlyconeogenesis - BIO 3110NaiomiBelum ada peringkat
- Corticosteroids: Saitoti S. Clinical Pharmacologist UdomDokumen33 halamanCorticosteroids: Saitoti S. Clinical Pharmacologist UdomZabron LuhendeBelum ada peringkat
- Gonococcal Infection in The Newborn - UpToDateDokumen13 halamanGonococcal Infection in The Newborn - UpToDateCarina ColtuneacBelum ada peringkat
- Medication Information For Parents and Teachers: Sertraline-ZoloftDokumen8 halamanMedication Information For Parents and Teachers: Sertraline-ZoloftCarina ColtuneacBelum ada peringkat
- Antidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsDokumen3 halamanAntidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsCarina ColtuneacBelum ada peringkat
- Zoloft Article 30 Referral Annex I II III IV - enDokumen52 halamanZoloft Article 30 Referral Annex I II III IV - enCarina ColtuneacBelum ada peringkat
- New Zealand Data Sheet: 1. Product NameDokumen23 halamanNew Zealand Data Sheet: 1. Product NameCarina ColtuneacBelum ada peringkat
- Study Guide Pueblo Aka Anasazi CultureDokumen5 halamanStudy Guide Pueblo Aka Anasazi CultureCarina ColtuneacBelum ada peringkat
- Neonatal Meningitis Due To Clostridium Neonatale: A Case ReportDokumen4 halamanNeonatal Meningitis Due To Clostridium Neonatale: A Case ReportCarina ColtuneacBelum ada peringkat
- Reading 1 Starter KitDokumen19 halamanReading 1 Starter KitCarina ColtuneacBelum ada peringkat
- Prevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaDokumen2 halamanPrevalence and Incidence' of Blindness Due To Age-Related Cataract in The Rural Areas of South AfricaCarina ColtuneacBelum ada peringkat
- Alterations in Energy Balance Following Exenatide AdministrationDokumen8 halamanAlterations in Energy Balance Following Exenatide AdministrationCarina ColtuneacBelum ada peringkat
- FertilityDokumen207 halamanFertilitypmotcBelum ada peringkat
- Biology: The Science of Life: Prepared By: Mrs. Ethel O. Cueto, RNDDokumen14 halamanBiology: The Science of Life: Prepared By: Mrs. Ethel O. Cueto, RNDnikki abalosBelum ada peringkat
- Corneal Reaction Towards Contact Lens Wear-2003poppyDokumen6 halamanCorneal Reaction Towards Contact Lens Wear-2003poppyFeiruz Hamid Umar BahasywenBelum ada peringkat
- WORKSHOP No 3Dokumen20 halamanWORKSHOP No 3Yainel RomeroBelum ada peringkat
- Penile US and Doppler USDokumen2 halamanPenile US and Doppler UShardrocker_2007Belum ada peringkat
- Language of Medicine 11th Edition Chabner Test BankDokumen25 halamanLanguage of Medicine 11th Edition Chabner Test BankRuthWilsoncoejg100% (46)
- Lesson 3.3Dokumen21 halamanLesson 3.3Claude Nathan AlidoBelum ada peringkat
- Active Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineDokumen52 halamanActive Principle: Lecture 10 Pharm Sci/Chem 177, University of California, IrvineVivian PhamBelum ada peringkat
- OPIANA CHRISTIAN JOSEPH - PulmonaryDisorderDokumen9 halamanOPIANA CHRISTIAN JOSEPH - PulmonaryDisorderChristian Joseph OpianaBelum ada peringkat
- Genetics - CMIDokumen177 halamanGenetics - CMI7ett_100% (1)
- Music Perception and Cognition: Development, Neural Basis, and Rehabilitative Use of MusicDokumen11 halamanMusic Perception and Cognition: Development, Neural Basis, and Rehabilitative Use of MusicAutes AG100% (1)
- SuffocationDokumen14 halamanSuffocationWan Gisca Ayu AstriniBelum ada peringkat
- General Biology Q4 M7Dokumen19 halamanGeneral Biology Q4 M7Mubin AbdulkarilBelum ada peringkat
- DEFINE Homeostasis, Osmoregulation, Thermoregulation and Excretion. 1. HomeostasisDokumen14 halamanDEFINE Homeostasis, Osmoregulation, Thermoregulation and Excretion. 1. HomeostasisStrange NazarBelum ada peringkat
- Deciphiring The Biology of M.TB WGS PDFDokumen27 halamanDeciphiring The Biology of M.TB WGS PDFSBTSRIRAMBelum ada peringkat
- Worksheet 1.2 Organelle QuizDokumen3 halamanWorksheet 1.2 Organelle QuizCyndel TindoyBelum ada peringkat
- 3.2 Cell Transport Ans PDFDokumen23 halaman3.2 Cell Transport Ans PDFtess_15Belum ada peringkat
- Rhopalocera (Butterfly) : FunctionsDokumen18 halamanRhopalocera (Butterfly) : FunctionsChris Anthony EdulanBelum ada peringkat
- The Heart AnatomyDokumen21 halamanThe Heart AnatomyLidia Dwi PutriBelum ada peringkat
- Checklist (PapSmear)Dokumen5 halamanChecklist (PapSmear)Sinung BawonoBelum ada peringkat
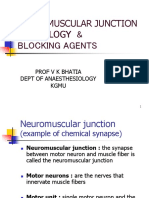
- Neuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuDokumen39 halamanNeuromuscular Junction Physiology & Blocking Agents: Prof V K Bhatia Dept of Anaesthesiology KgmuAthira S MadhuBelum ada peringkat
- Anchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFDokumen6 halamanAnchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFsolodont1Belum ada peringkat
- Chapter - 005 Interdependent Body SystemsDokumen46 halamanChapter - 005 Interdependent Body SystemsTina VargheseBelum ada peringkat
- Bovine Theileriosis: A Case Study Survey at Chitwan, NepalDokumen28 halamanBovine Theileriosis: A Case Study Survey at Chitwan, NepalJibachha ShahBelum ada peringkat
- AutopsyDokumen24 halamanAutopsyRoberto Giorgio N. Pacheco100% (1)
- Respiratory Tract Infection PDFDokumen64 halamanRespiratory Tract Infection PDFMaretah TaufahBelum ada peringkat
- HTTPS://WWW - Scribd.com/presentation/332117871/mga Uri NG Tekstong ImpormatiboDokumen2 halamanHTTPS://WWW - Scribd.com/presentation/332117871/mga Uri NG Tekstong ImpormatiboRegine AbilarBelum ada peringkat
- Brosur Intensa GoDokumen8 halamanBrosur Intensa GoAnonymous tbJ24554Belum ada peringkat
- Characterization of CarbohydratesDokumen3 halamanCharacterization of CarbohydratesHyvieBelum ada peringkat