Anda mungkin juga menyukai
- Primary ImpressionDokumen17 halamanPrimary ImpressionJewana J. GhazalBelum ada peringkat
- Diagnostic Cast and Its UsesDokumen12 halamanDiagnostic Cast and Its UsesKumarBelum ada peringkat
- Priliminary Impression DR - Ashraf GebreelDokumen37 halamanPriliminary Impression DR - Ashraf Gebreelapi-19967864Belum ada peringkat
- DentistryDokumen104 halamanDentistrypriyankaBelum ada peringkat
- Ocular Prosthesis PDFDokumen2 halamanOcular Prosthesis PDFBrianBelum ada peringkat
- Factors Affecting Selection of Artificial TeethDokumen7 halamanFactors Affecting Selection of Artificial TeethSora Tensai100% (1)
- Primary ImpressionDokumen18 halamanPrimary ImpressionJewana J. Ghazal67% (3)
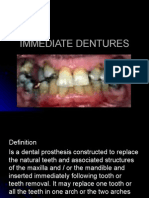
- Immediate DenturesDokumen23 halamanImmediate DenturesWael FahadBelum ada peringkat
- Fixed Partial DentureDokumen2 halamanFixed Partial DentureGabriel Chua PaderonBelum ada peringkat
- Fabrication of Suction-Effective Mandibular DenturesDokumen36 halamanFabrication of Suction-Effective Mandibular DenturesSharlene OngBelum ada peringkat
- Impression Materials / Orthodontic Courses by Indian Dental AcademyDokumen52 halamanImpression Materials / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Management of Acquired Maxillary Defects Partially Edentlous PDFDokumen129 halamanManagement of Acquired Maxillary Defects Partially Edentlous PDFRamy Khalifa AshmawyBelum ada peringkat
- Prosthetic 6Dokumen5 halamanProsthetic 6زهراء فاضل اجبير فعيلBelum ada peringkat
- Biomatric Approach For Complete Denture DesignDokumen18 halamanBiomatric Approach For Complete Denture Designفواز نميرBelum ada peringkat
- Overdenture 140503222227 Phpapp01Dokumen107 halamanOverdenture 140503222227 Phpapp01TatsamYadavBelum ada peringkat
- Biological Considerations of Orientation, Vertical and Horizontal Jaw Relations in Complete Denture-First PartDokumen43 halamanBiological Considerations of Orientation, Vertical and Horizontal Jaw Relations in Complete Denture-First PartArunBelum ada peringkat
- GENERAL PRINCIPLES OF SHADE SELECTION LDDokumen3 halamanGENERAL PRINCIPLES OF SHADE SELECTION LDrasagna reddyBelum ada peringkat
- Development of Dentition & OcclusionDokumen109 halamanDevelopment of Dentition & OcclusionSyed Mohammad Osama Ahsan100% (1)
- Classification and Composition of Resilient Lining Materials (RLMS)Dokumen5 halamanClassification and Composition of Resilient Lining Materials (RLMS)Sonia LeeBelum ada peringkat
- Tissue Management & Impression TechniquesDokumen49 halamanTissue Management & Impression Techniquesapi-1984040480% (5)
- 2014 Table Clinic InstructionsDokumen19 halaman2014 Table Clinic InstructionsMaria Mercedes LeivaBelum ada peringkat
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDari EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideBelum ada peringkat
- Final Year Lecture 11 AugustDokumen78 halamanFinal Year Lecture 11 Augustprostho deptBelum ada peringkat
- PBL Cephalometry DentistryDokumen15 halamanPBL Cephalometry DentistryZYenHoBelum ada peringkat
- Prepared By:: Dr. Ranjeet Kumar ChaudharyDokumen22 halamanPrepared By:: Dr. Ranjeet Kumar ChaudharyDrRanjeet Kumar ChaudharyBelum ada peringkat
- Adel Lecture 7&8 Post Crown Part1Dokumen0 halamanAdel Lecture 7&8 Post Crown Part1Ravik FidayatikaBelum ada peringkat
- Complete Denture Complaints IIDokumen65 halamanComplete Denture Complaints IIbkprosthoBelum ada peringkat
- Pontic SeminarDokumen40 halamanPontic Seminarankita sethiBelum ada peringkat
- Elastics in Ortho IiDokumen29 halamanElastics in Ortho IiSurabhi SaxenaBelum ada peringkat
- Partial Coverage RetainersDokumen55 halamanPartial Coverage RetainersKhalid Aly El Banna0% (2)
- Examination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsDokumen73 halamanExamination, Diagnosis and Treatment Planning For Edentulous or Partially Edentulous PatientsMohamedBelum ada peringkat
- Retention in Complete DenturesDokumen10 halamanRetention in Complete Dentures李潮忠Belum ada peringkat
- Single Complete DenturesDokumen20 halamanSingle Complete DenturesDeepthi RajeshBelum ada peringkat
- Retention Support Stability CDDokumen53 halamanRetention Support Stability CDAshraf GebreelBelum ada peringkat
- Royal London Space AnalysisDokumen47 halamanRoyal London Space AnalysisYusra ShaukatBelum ada peringkat
- Twin BlockDokumen124 halamanTwin Blockrama deviBelum ada peringkat
- Flat Ridgel Impression TechniqueDokumen4 halamanFlat Ridgel Impression TechniquerekabiBelum ada peringkat
- Articulators and Articulation.Dokumen21 halamanArticulators and Articulation.colltfrankBelum ada peringkat
- C&B 12 RBBDokumen89 halamanC&B 12 RBBNam BuiBelum ada peringkat
- Oper-Notes-Anterior Direct Composite Restorations Lec02 (Dina Elqassas) - Samar Bebers PDFDokumen8 halamanOper-Notes-Anterior Direct Composite Restorations Lec02 (Dina Elqassas) - Samar Bebers PDFMostafa Afifi AliBelum ada peringkat
- Lec1 - Bridge (Fixed Partial DentureDokumen9 halamanLec1 - Bridge (Fixed Partial Dentureكاظم عبد الحسينBelum ada peringkat
- Requirements of An Articulator Corident CSA 400Dokumen16 halamanRequirements of An Articulator Corident CSA 400pratik guptaBelum ada peringkat
- Impressions: Presented By: Dr. Mansi Sharma Department of Prosthodontics Crown and Bridge PG1 YearDokumen61 halamanImpressions: Presented By: Dr. Mansi Sharma Department of Prosthodontics Crown and Bridge PG1 YearshailjaBelum ada peringkat
- Solutions Chapter 9Dokumen34 halamanSolutions Chapter 9reloadedmemoryBelum ada peringkat
- Section 019 EstheticsDokumen10 halamanSection 019 EstheticsMohammed LafiBelum ada peringkat
- Lec 4 Prosthodontics PDFDokumen7 halamanLec 4 Prosthodontics PDFmustafa7calligrapherBelum ada peringkat
- Post Dam AreaDokumen2 halamanPost Dam ArearazasiddiqueBelum ada peringkat
- Pangan, Maria Elaine S. Inlay Onlay GoldDokumen6 halamanPangan, Maria Elaine S. Inlay Onlay GoldErika PanganBelum ada peringkat
- ImpressionDokumen7 halamanImpressionAnnisa Nur AmalaBelum ada peringkat
- Endodontic Insruments-1Dokumen114 halamanEndodontic Insruments-1Rimy Singh100% (1)
- The Function and Importance of Incisal Guidance in Oral RehabilitationDokumen14 halamanThe Function and Importance of Incisal Guidance in Oral RehabilitationPablo Gutiérrez Da VeneziaBelum ada peringkat
- Tooth Preparation For Full Veneer Crowns SuchiDokumen76 halamanTooth Preparation For Full Veneer Crowns SuchisaptoBelum ada peringkat
- Jaw Relation Record, Lec 6Dokumen12 halamanJaw Relation Record, Lec 6JustDen09100% (1)
- Ceph (2) / Orthodontic Courses by Indian Dental AcademyDokumen112 halamanCeph (2) / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Complete Denture JourneyDokumen30 halamanComplete Denture JourneysapnaBelum ada peringkat
- Biometric - Approach in CDDokumen13 halamanBiometric - Approach in CDmarwaBelum ada peringkat
- 1 s2.0 S002239131360030X MainDokumen6 halaman1 s2.0 S002239131360030X MainAmar Bhochhibhoya100% (1)
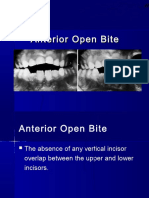
- Anterior Open BiteDokumen34 halamanAnterior Open BiteAbdullah100% (1)
- Clinical Cases in Restorative and Reconstructive DentistryDari EverandClinical Cases in Restorative and Reconstructive DentistryPenilaian: 5 dari 5 bintang5/5 (1)
- Restorative Space and Occlusal Evaluation RPDDokumen48 halamanRestorative Space and Occlusal Evaluation RPDKulashekar ReddyBelum ada peringkat
- MCQ in RPDDokumen10 halamanMCQ in RPDIbrahim Ramadan Eltorky91% (11)
- Esthetic Localized Soft Tissue Ridge Augmentation in A Fixed Partial Denture A Case Report PDFDokumen3 halamanEsthetic Localized Soft Tissue Ridge Augmentation in A Fixed Partial Denture A Case Report PDFAmar Bhochhibhoya0% (1)
- Tallgren1972 PDFDokumen13 halamanTallgren1972 PDFgermanpuig100% (1)
- The Neutral Zone Concept in Complete DentureDokumen122 halamanThe Neutral Zone Concept in Complete Denturevahini niharikaBelum ada peringkat
- Impression Making in Complete DentureDokumen128 halamanImpression Making in Complete DentureBharanijaBelum ada peringkat
- Clinical Evaluation of Failures of Removable Partial DenturesDokumen7 halamanClinical Evaluation of Failures of Removable Partial DenturesOctavian TaviBelum ada peringkat
- RCDSO Guidelines Implant DentistryDokumen16 halamanRCDSO Guidelines Implant DentistrydoctorlupuBelum ada peringkat
- Flangeless Cast Partial DentureDokumen5 halamanFlangeless Cast Partial DentureDeasiree100% (1)
- Krok 2 Stomatology: Test Items For Licensing ExaminationDokumen30 halamanKrok 2 Stomatology: Test Items For Licensing ExaminationjimmyBelum ada peringkat
- Using Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionDokumen15 halamanUsing Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionAlfred OrozcoBelum ada peringkat
- MFD Part 2 Exam Held in JUST, Jordan On 12-2013Dokumen2 halamanMFD Part 2 Exam Held in JUST, Jordan On 12-2013sohaib197Belum ada peringkat
- Dentist Protocol March 2018 - CurrentDokumen12 halamanDentist Protocol March 2018 - CurrentZomba ZombariraBelum ada peringkat
- ObturatorsDokumen162 halamanObturatorsTaran67% (3)
- Snap On Smile Todays Multi Purpose Restorative ApplianceDokumen94 halamanSnap On Smile Todays Multi Purpose Restorative Applianceamit100% (2)
- Maxillary Major ConnectorsDokumen9 halamanMaxillary Major ConnectorsAsbiKirkkBelum ada peringkat
- Telescopic DentureDokumen5 halamanTelescopic DentureDrRahul Puri GoswamiBelum ada peringkat
- ReferensiDokumen4 halamanReferensiluluBelum ada peringkat
- Anterior Tooth SelectionDokumen54 halamanAnterior Tooth SelectionashoorocksBelum ada peringkat
- Ortho Bone ScrewDokumen17 halamanOrtho Bone ScrewmedicalcenterBelum ada peringkat
- Removable PARTIAL DENTURE THEORY AND PRACTICEDokumen643 halamanRemovable PARTIAL DENTURE THEORY AND PRACTICEMostafa Fayad94% (16)
- Futher Aspects of Design For Distal Extension RemovableDokumen5 halamanFuther Aspects of Design For Distal Extension RemovableLisset MaritzaBelum ada peringkat
- RPD CourseDokumen39 halamanRPD CourseJackson khoBelum ada peringkat
- LoDokumen43 halamanLoAwani GuptaBelum ada peringkat
- Ridge Augmentation in Implant Dentistry PDFDokumen19 halamanRidge Augmentation in Implant Dentistry PDFAngelina100% (1)
- Fixed Partial Dentures PPT For StudentsDokumen151 halamanFixed Partial Dentures PPT For Studentsduracell1950% (4)
- Ort Stom PDFDokumen100 halamanOrt Stom PDFaliolveroBelum ada peringkat
- B.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDDokumen7 halamanB.A.,D.D.S.,M.S.D. : Herbert Werdlow, Bethesda, MDMuchlis Fauzi EBelum ada peringkat
- Interdisciplinary Treat Planning ChapterDokumen56 halamanInterdisciplinary Treat Planning ChapterJulio César Huayllasco de la Cruz0% (1)
- Principle Partial Dent DesignDokumen37 halamanPrinciple Partial Dent DesignSanBelum ada peringkat