Anda mungkin juga menyukai
- Management of Tuberculosis: A guide for clinicians (eBook edition)Dari EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Belum ada peringkat
- Wounds and Tissue RepairDokumen4 halamanWounds and Tissue RepairMuhammad Mohsin Ali Dynamo0% (1)
- T Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramDokumen3 halamanT Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramKhaled Shaheen100% (1)
- Surgery Mcqs PDFDokumen43 halamanSurgery Mcqs PDFjcc50% (2)
- TrumaDokumen13 halamanTrumaShrestha Anjiv100% (1)
- 1 - Pedia2le1 PDFDokumen10 halaman1 - Pedia2le1 PDFLancelot BritaniaBelum ada peringkat
- Preoperative Preparation of The Surgical PatientDokumen33 halamanPreoperative Preparation of The Surgical PatientPrincewill SeiyefaBelum ada peringkat
- UlcersDokumen2 halamanUlcersAamir BugtiBelum ada peringkat
- Aetiology, Pathology and Management of Enterocutaneous FistulaDokumen34 halamanAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (1)
- Community Diagnosis: Prepared and Comfiled By: Juanaly Almonte-Badiola, RN, ManDokumen87 halamanCommunity Diagnosis: Prepared and Comfiled By: Juanaly Almonte-Badiola, RN, Manjuanamay30gmailcomBelum ada peringkat
- اسئله جراحه عامه سنوات سابقه امتحان الامتيازDokumen110 halamanاسئله جراحه عامه سنوات سابقه امتحان الامتيازZaid ZayedBelum ada peringkat
- Surgical InfectionsDokumen54 halamanSurgical Infectionsmanish shresthaBelum ada peringkat
- Surgery I & Ortho PDFDokumen124 halamanSurgery I & Ortho PDFUmangBelum ada peringkat
- Cardiothoracic SurgeryDokumen2 halamanCardiothoracic Surgeryc3145848Belum ada peringkat
- Surgery UpcamDokumen11 halamanSurgery UpcamArchie DuqueBelum ada peringkat
- Test For Mci ScreeningDokumen43 halamanTest For Mci ScreeningGulamenasir AhmednasirwalaBelum ada peringkat
- Pressure UlcersDokumen38 halamanPressure UlcersRadwa EbedBelum ada peringkat
- MCQ On NeurologyDokumen2 halamanMCQ On NeurologynamsoBelum ada peringkat
- Introduction To SurgeryDokumen45 halamanIntroduction To SurgeryBea Marie Eclevia100% (1)
- Healing Mcqs ExplainedDokumen3 halamanHealing Mcqs Explainedsaad awanBelum ada peringkat
- Mcqs Faculty of General Medicine VI YearDokumen110 halamanMcqs Faculty of General Medicine VI YearAbdimajiid100% (2)
- Screenshot 2023-01-22 at 19.25.23Dokumen49 halamanScreenshot 2023-01-22 at 19.25.23Lika BukhaidzeBelum ada peringkat
- Polytrauma - A Team ApproachDokumen52 halamanPolytrauma - A Team ApproachparkmickybooBelum ada peringkat
- Robbins Ch. 19 The Pancreas Review QuestionsDokumen3 halamanRobbins Ch. 19 The Pancreas Review QuestionsPA2014100% (1)
- Connective Tissue LesionsDokumen285 halamanConnective Tissue LesionsRwskhans KhanBelum ada peringkat
- Midyear 2009 GS Office 2003Dokumen100 halamanMidyear 2009 GS Office 2003Ahmad Alnemare100% (2)
- Surgical Site InfectionsDokumen22 halamanSurgical Site InfectionsSheryl DurrBelum ada peringkat
- Gastrointestinal SurgeryDokumen78 halamanGastrointestinal Surgeryjjmail100% (1)
- Surgery MCQDokumen33 halamanSurgery MCQFan EliBelum ada peringkat
- About 70% of All Sensory Information Reaches The Brain Through The EyesDokumen127 halamanAbout 70% of All Sensory Information Reaches The Brain Through The Eyesjoan olanteBelum ada peringkat
- Gyne ObsqsDokumen30 halamanGyne ObsqsMarsFriendBelum ada peringkat
- Combined Okell NotesDokumen202 halamanCombined Okell Notessameeramw100% (5)
- Syllabus of MD General MedicineDokumen5 halamanSyllabus of MD General Medicine2shubhoBelum ada peringkat
- Fraility: Presence of Risk Factors Reduced Resilience FrailtyDokumen4 halamanFraility: Presence of Risk Factors Reduced Resilience FrailtyFatin Nurina Mohd Nazemi100% (1)
- Managemet PT SafetyDokumen296 halamanManagemet PT SafetyCHALIE MEQUBelum ada peringkat
- Head Injury 2Dokumen47 halamanHead Injury 2drvishal bhattBelum ada peringkat
- Nasopharyngeal CarcinomaDokumen44 halamanNasopharyngeal CarcinomapopoyingBelum ada peringkat
- BleedingDokumen14 halamanBleedingRhomizal MazaliBelum ada peringkat
- Acute Pancreatitis Case PresDokumen29 halamanAcute Pancreatitis Case Preskristine keen buanBelum ada peringkat
- Slides 2 - Wounds, UlcersDokumen80 halamanSlides 2 - Wounds, UlcersCWT2010Belum ada peringkat
- Neuro PDFDokumen12 halamanNeuro PDFVishnu Krsh100% (1)
- Copy Surgery MCQDokumen12 halamanCopy Surgery MCQAbubakar JallohBelum ada peringkat
- Test - 4 MCQsDokumen3 halamanTest - 4 MCQsعايشاة زارينBelum ada peringkat
- Orbital TumorsDokumen12 halamanOrbital Tumorsamae85100% (1)
- MG Test1Dokumen7 halamanMG Test1CherryBelum ada peringkat
- Metabolic Response To TraumaDokumen52 halamanMetabolic Response To TraumaAnil BasnetBelum ada peringkat
- Head InjuryDokumen22 halamanHead InjuryNguyễn Ly100% (1)
- Osteoarthritis: T Person's of Developing Osteoarthritis. It IncludesDokumen5 halamanOsteoarthritis: T Person's of Developing Osteoarthritis. It IncludesLove Shery SabrosoBelum ada peringkat
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADokumen31 halamanIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangBelum ada peringkat
- Patellar FracturesDokumen26 halamanPatellar FracturesDavid VillanuevaBelum ada peringkat
- B) Bilateral Grade 1 Varicocele.: UrologyDokumen12 halamanB) Bilateral Grade 1 Varicocele.: UrologyPapa RatxiBelum ada peringkat
- Sexual Medicine ETRDokumen65 halamanSexual Medicine ETRkhplwakabidullah148Belum ada peringkat
- ATLS and Orthopaedic TraumaDokumen67 halamanATLS and Orthopaedic TraumayasserBelum ada peringkat
- Fracture in ChildrenDokumen40 halamanFracture in ChildrenMutiara Jihad100% (1)
- MCQ For PracticeDokumen33 halamanMCQ For PracticeMandela KibiritiBelum ada peringkat
- Clinical NeurologyDokumen288 halamanClinical NeurologyWeronika Tomaszczuk-KłakBelum ada peringkat
- FPM FFPMRCA Example Questions 2016Dokumen15 halamanFPM FFPMRCA Example Questions 2016hawraa tarhiniBelum ada peringkat
- Para PhimosisDokumen9 halamanPara PhimosisNazurah Azmira100% (1)
- The Ultimate Emergency Medicine Guide Ebook PDF VersionDokumen61 halamanThe Ultimate Emergency Medicine Guide Ebook PDF Versiontom.dimaggio515100% (35)
- N2ODokumen2 halamanN2Ochanaish6Belum ada peringkat
- Oxford Handbooks Download LinkDokumen5 halamanOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- Dental MCQ StudyDokumen28 halamanDental MCQ Studychanaish6Belum ada peringkat
- General Anesthesia PDFDokumen8 halamanGeneral Anesthesia PDFchanaish6Belum ada peringkat
- Sle Part 3Dokumen12 halamanSle Part 3chanaish6Belum ada peringkat
- 1Dokumen8 halaman1chanaish6Belum ada peringkat
- My Saudhi Council ExamDokumen15 halamanMy Saudhi Council Examchanaish6Belum ada peringkat
- McqsDokumen8 halamanMcqschanaish6Belum ada peringkat
- Indication For Open Reduction of Condylar Fractures Zide and KentDokumen10 halamanIndication For Open Reduction of Condylar Fractures Zide and Kentchanaish60% (1)
- Infection ControlDokumen5 halamanInfection Controlchanaish6Belum ada peringkat
- ARMAMENTARIUMDokumen105 halamanARMAMENTARIUMchanaish6Belum ada peringkat
- Role of Collagen in Vestibuloplasty - A Comparative StudyDokumen2 halamanRole of Collagen in Vestibuloplasty - A Comparative Studychanaish6Belum ada peringkat
- Compound Complex Odontoma An Important Clinical EntityDokumen6 halamanCompound Complex Odontoma An Important Clinical Entitychanaish6Belum ada peringkat
- Letters To EditorDokumen2 halamanLetters To Editorchanaish6Belum ada peringkat
- Anatomy of Brain and Function - NaemaDokumen7 halamanAnatomy of Brain and Function - NaemaHana Naema ZelinBelum ada peringkat
- Test 3 SCRIPTDokumen6 halamanTest 3 SCRIPT52000854Belum ada peringkat
- QP-005 Training ProcessDokumen3 halamanQP-005 Training Processesraa asemBelum ada peringkat
- Prep 4 Post LabDokumen2 halamanPrep 4 Post LabKate MendozaBelum ada peringkat
- Nevid CH14 TBDokumen71 halamanNevid CH14 TBAngela MarisBelum ada peringkat
- History of Nursing in The Philippines: Early Beliefs & PracticesDokumen2 halamanHistory of Nursing in The Philippines: Early Beliefs & Practicesjared gabuleBelum ada peringkat
- Physiology of Digestive SystemDokumen70 halamanPhysiology of Digestive SystemVincent SerBelum ada peringkat
- Dr. Diana Mostafa Abo El OlaDokumen68 halamanDr. Diana Mostafa Abo El Olasohaib natshehBelum ada peringkat
- Health Promotion and MaintenanceDokumen3 halamanHealth Promotion and MaintenanceYuuki Chitose (tai-kun)Belum ada peringkat
- SweetDachs Sales Contract-15Dokumen3 halamanSweetDachs Sales Contract-15Katelyn ShirkBelum ada peringkat
- General Science and AbilityDokumen4 halamanGeneral Science and AbilityUsra RasoolBelum ada peringkat
- (Rickie Solinger) Reproductive Politics What EverDokumen236 halaman(Rickie Solinger) Reproductive Politics What EverhercuBelum ada peringkat
- Practice Test A3Dokumen8 halamanPractice Test A3Khang Nguyen TienBelum ada peringkat
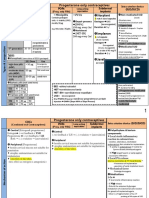
- Norplant: Progesterone Only ContraceptivesDokumen9 halamanNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyBelum ada peringkat
- EpicondilteDokumen7 halamanEpicondilteRicardo fariaBelum ada peringkat
- VapeDokumen2 halamanVapeVanessa MendozaBelum ada peringkat
- IARCDokumen868 halamanIARCmarcosiqBelum ada peringkat
- Concept of Ovulation in AyurvedaDokumen6 halamanConcept of Ovulation in Ayurvedasan MunBelum ada peringkat
- The Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of AsiaDokumen28 halamanThe Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of Asiaojay_88Belum ada peringkat
- Hemet City Manager Christopher LopezDokumen15 halamanHemet City Manager Christopher LopezHemetUpdatesBelum ada peringkat
- HSE Lecture NotesDokumen10 halamanHSE Lecture NotesAndreBelum ada peringkat
- Reliability MedEl CI-3d98 PDFDokumen6 halamanReliability MedEl CI-3d98 PDFneculavBelum ada peringkat
- USAR EquipmentDokumen41 halamanUSAR EquipmentSérgio RibeiroBelum ada peringkat
- Basics of Mechanical VentilationDokumen5 halamanBasics of Mechanical Ventilationruhaina malikBelum ada peringkat
- Market Development Approaches Scoping Report: Authors: Elizabeth Gardiner, Ditlev Schwanenflugel & Cheri GraceDokumen64 halamanMarket Development Approaches Scoping Report: Authors: Elizabeth Gardiner, Ditlev Schwanenflugel & Cheri GraceAjith AjithBelum ada peringkat
- International Journal of Dental Science and Innovative Research (IJDSIR)Dokumen7 halamanInternational Journal of Dental Science and Innovative Research (IJDSIR)yusfaBelum ada peringkat
- Frontliners HirarcDokumen8 halamanFrontliners HirarcSitiAliahBelum ada peringkat
- Neuromitos PDFDokumen9 halamanNeuromitos PDFAriel JaraBelum ada peringkat
- Medical ReportDokumen1 halamanMedical ReportamrulBelum ada peringkat
- InfographicDokumen4 halamanInfographicJustin TanBelum ada peringkat