Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- New Hope For A Cure To Liver CirrhosisDokumen2 halamanNew Hope For A Cure To Liver Cirrhosissina_bopol100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The JCI Big Book of ChecklistDokumen150 halamanThe JCI Big Book of ChecklistMiguel Angel Chávez88% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Perspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Dokumen2 halamanPerspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Tahi GuzmánBelum ada peringkat
- Dr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Dokumen73 halamanDr. Robert Tirtowijoyo (Paediatric Condition) Inggris UMJ Maret 2008Muhamad Agung SupriyantoBelum ada peringkat
- Nabh Training Topics For All The Departmental StaffDokumen4 halamanNabh Training Topics For All The Departmental StaffMr. R. Ramesh75% (8)
- MAHONY, Patrick - The Boundaries of Free AssociationDokumen34 halamanMAHONY, Patrick - The Boundaries of Free AssociationPelículasVeladasBelum ada peringkat
- NCP ConstipationDokumen3 halamanNCP ConstipationNika LoBelum ada peringkat
- Practice Test QuestionsDokumen14 halamanPractice Test QuestionsFilipino Nurses CentralBelum ada peringkat
- FryetteDokumen2 halamanFryetteSaba KhanBelum ada peringkat
- ADA Guidelines For Infection Control 3rd EdDokumen56 halamanADA Guidelines For Infection Control 3rd Edaprmaster100% (2)
- Healing ArchitectureDokumen5 halamanHealing ArchitectureSUDHAKARMANI100% (2)
- Conduct DisorderDokumen7 halamanConduct DisorderSenka Nenadov100% (1)
- Disseminated Intravascular Coagulopathy Dic 1 1Dokumen25 halamanDisseminated Intravascular Coagulopathy Dic 1 1api-394684626Belum ada peringkat
- Confidence IntervalDokumen1 halamanConfidence IntervalFelix Ray DumaganBelum ada peringkat
- DyalisisDokumen24 halamanDyalisisAbdulla Abu EidBelum ada peringkat
- Jurnal Rujukan KuesionerDokumen10 halamanJurnal Rujukan KuesionerMiss BerlyantiBelum ada peringkat
- General Dentistry Exam References and ContentDokumen2 halamanGeneral Dentistry Exam References and ContentKannan DevBelum ada peringkat
- Dermatitis Perioral 2015Dokumen7 halamanDermatitis Perioral 2015Carlos Augusto Morales ChaconBelum ada peringkat
- Basal GangliaDokumen48 halamanBasal GangliaMudassar Roomi100% (1)
- Fresh Frozen Plasma (FFP) Dosage: Calculations For One Adult Therapeutic Dose FFPDokumen1 halamanFresh Frozen Plasma (FFP) Dosage: Calculations For One Adult Therapeutic Dose FFPKamran Afzal100% (1)
- Agen HematinikDokumen77 halamanAgen HematinikErinaGeraldiBelum ada peringkat
- Chiari Malformation / Syringomyelia SchemeDokumen4 halamanChiari Malformation / Syringomyelia SchemeMihai SavescuBelum ada peringkat
- Renal DisordersDokumen77 halamanRenal Disorderslorelee_espaldon100% (1)
- Expert Consensus On The Desirable Characteristics of Review Criteria For Improvement of Health Care QualityDokumen6 halamanExpert Consensus On The Desirable Characteristics of Review Criteria For Improvement of Health Care Qualityujangketul62Belum ada peringkat
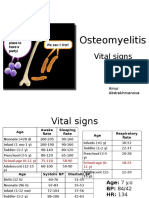
- PBL 2 - OsteomyelitisDokumen10 halamanPBL 2 - OsteomyelitisAinur AbdrakhmanovaBelum ada peringkat
- Comprehension Book Grade 12Dokumen66 halamanComprehension Book Grade 12milkovicius0% (3)
- Medical CenterDokumen38 halamanMedical CenterKhea Micole MayBelum ada peringkat
- IPOL Package InsertDokumen28 halamanIPOL Package InsertHeather X RhodesBelum ada peringkat
- Role Play Moving Patient From Bed To WheelchairDokumen2 halamanRole Play Moving Patient From Bed To WheelchairDevina RahmaBelum ada peringkat
- Children-Mental Health-Facts-NamiDokumen1 halamanChildren-Mental Health-Facts-Namiapi-298799918Belum ada peringkat