Anda mungkin juga menyukai
- Distal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiDokumen5 halamanDistal Biceps Repair Rehabilitation Protocol by Tendayi MutsopotsiPhysiotherapy Care SpecialistsBelum ada peringkat
- Total Hip Arthroplasty PDFDokumen10 halamanTotal Hip Arthroplasty PDFWindy ZeniccBelum ada peringkat
- Median Nerve Injury Causes Ape Hand DeformityDokumen16 halamanMedian Nerve Injury Causes Ape Hand Deformitymedical- physio classesBelum ada peringkat
- Objective Assessment of Spinal Cord InjuryDokumen25 halamanObjective Assessment of Spinal Cord InjuryYangBelum ada peringkat
- Orthosisofhandppt 181202162551Dokumen65 halamanOrthosisofhandppt 181202162551Khageswar SamalBelum ada peringkat
- Gait Analysis GuideDokumen4 halamanGait Analysis GuideMokibul100% (1)
- Lower Extremity Conditions Part 4 NPTE FF LSPDokumen10 halamanLower Extremity Conditions Part 4 NPTE FF LSPDBelum ada peringkat
- Spinal Cord InjuryDokumen39 halamanSpinal Cord InjuryrahatBelum ada peringkat
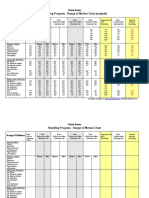
- Standing Program - Range of Motion Chart (Sample) : Client NameDokumen2 halamanStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezBelum ada peringkat
- Shoulder Exam Guide: Inspection, Palpation, ROM, Neurovascular, Special TestsDokumen12 halamanShoulder Exam Guide: Inspection, Palpation, ROM, Neurovascular, Special Testsckyew64Belum ada peringkat
- Frozen ShoulderDokumen44 halamanFrozen ShoulderEspers BluesBelum ada peringkat
- Examine Cervical Spine Range MotionDokumen16 halamanExamine Cervical Spine Range MotionlecturioBelum ada peringkat
- Primary and Secondary Adhesive Capsulitis Etiology, Stages, Signs, Tests and ManagementDokumen8 halamanPrimary and Secondary Adhesive Capsulitis Etiology, Stages, Signs, Tests and ManagementVanessa Yvonne Gurtiza100% (1)
- Proc RangeOfMotionDokumen4 halamanProc RangeOfMotionSri KuspartianingsihBelum ada peringkat
- Shoulder Knee WristDokumen110 halamanShoulder Knee Wriststevebravo81100% (1)
- MMT 6-1Dokumen20 halamanMMT 6-1Mughal ZadiiBelum ada peringkat
- Management L Low Back PainDokumen7 halamanManagement L Low Back PainelsyamelindaBelum ada peringkat
- RomDokumen6 halamanRomPrivat Etavirp0% (1)
- Lower Extremity Special TestsDokumen16 halamanLower Extremity Special TestsAlyssa BatasBelum ada peringkat
- Special Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With ADokumen32 halamanSpecial Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With AnatkwqBelum ada peringkat
- Lateral Epicondylitis: ST NDDokumen2 halamanLateral Epicondylitis: ST NDMuhammad Ucuk100% (1)
- Glassgow Coma Scale and Rancho Los AmigosDokumen17 halamanGlassgow Coma Scale and Rancho Los AmigosHEMA CHANDRANBelum ada peringkat
- Exit Project Workbook Complete Draft 2Dokumen2 halamanExit Project Workbook Complete Draft 2vladBelum ada peringkat
- AAOS2002 ShoulderDokumen70 halamanAAOS2002 ShoulderHéctor Pando SánchezBelum ada peringkat
- CAPR Blueprint enDokumen9 halamanCAPR Blueprint enramandeepkaurBelum ada peringkat
- JOSPT Shoulder Pain and Mobility Deficitis Adhesive Capsulitis PDFDokumen33 halamanJOSPT Shoulder Pain and Mobility Deficitis Adhesive Capsulitis PDFAbdul Wahid ShaikhBelum ada peringkat
- PT Initial EvaluationDokumen6 halamanPT Initial EvaluationJudith Bartolo100% (1)
- Hemiarthroplasty Hip - Apr20Dokumen10 halamanHemiarthroplasty Hip - Apr20Shalu OjhaBelum ada peringkat
- Saunders Q&A ReviewDokumen368 halamanSaunders Q&A ReviewDeepakBelum ada peringkat
- SCI Acute Care and Rehabilitation PT 2009Dokumen265 halamanSCI Acute Care and Rehabilitation PT 2009api-3822828Belum ada peringkat
- Epicondylitis, Lateral: (Tennis Elbow)Dokumen6 halamanEpicondylitis, Lateral: (Tennis Elbow)ArieZta Kautsar RahmanBelum ada peringkat
- Orthosis Dan ProsthesisDokumen39 halamanOrthosis Dan ProsthesisdimasBelum ada peringkat
- Manual Muscle Testing: Grade Value DescriptionDokumen40 halamanManual Muscle Testing: Grade Value Descriptionjoanna gurtizaBelum ada peringkat
- Upper Extremity Rom NormsDokumen3 halamanUpper Extremity Rom Normsapi-336924644Belum ada peringkat
- Tennis ElbowDokumen13 halamanTennis ElbowPadma PadalBelum ada peringkat
- Access NPTE Review Lecture OutlineDokumen12 halamanAccess NPTE Review Lecture OutlinecutlaborcostBelum ada peringkat
- Rehabilitation protocol for mallet finger and zone injuriesDokumen18 halamanRehabilitation protocol for mallet finger and zone injuriesaparnaBelum ada peringkat
- Physiotherapy Management of Tennis Elbow................ ArticleDokumen5 halamanPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiBelum ada peringkat
- Balance TestDokumen21 halamanBalance TestSyazaWajihahZulkefliBelum ada peringkat
- Hip Application SolutionsDokumen3 halamanHip Application SolutionsDBelum ada peringkat
- Evaluation of The Hand!Dokumen84 halamanEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- Achilles Pain, Stiffness, and Muscle Power Deficits - Midportion Achilles Tendinopathy Revision 2018Dokumen38 halamanAchilles Pain, Stiffness, and Muscle Power Deficits - Midportion Achilles Tendinopathy Revision 2018Marcus Dos SantosBelum ada peringkat
- HMP (Hot Moist Pack W. Fluido Therapy)Dokumen17 halamanHMP (Hot Moist Pack W. Fluido Therapy)yamhtur_17100% (1)
- KMC Dept of Orthopaedics Floor Reaction OrthosisDokumen5 halamanKMC Dept of Orthopaedics Floor Reaction OrthosischinmayghaisasBelum ada peringkat
- PT Neuro Intro NotesDokumen13 halamanPT Neuro Intro NotesSusan K100% (1)
- Joint ROMDokumen2 halamanJoint ROMdr_gentel19Belum ada peringkat
- Development Chart For BookletDokumen13 halamanDevelopment Chart For BookletzapelBelum ada peringkat
- Jospt LBPDokumen58 halamanJospt LBPHelda PurwaningtiyasBelum ada peringkat
- Shoulder Dislocation DraftDokumen26 halamanShoulder Dislocation Drafthusnajihah18Belum ada peringkat
- Upper Limb Orthosis - Dr. Bhaskarananda KumarDokumen33 halamanUpper Limb Orthosis - Dr. Bhaskarananda KumarsudiptomukherjeeBelum ada peringkat
- Classification of Upper Limb OrthosesDokumen16 halamanClassification of Upper Limb Orthoseszoha hassanBelum ada peringkat
- Carpal Tunnel Syndrome FinalDokumen4 halamanCarpal Tunnel Syndrome Finalcatherine_suganob6496100% (2)
- HEAD NECK BACK SPINE SPECIAL TESTS December 2022Dokumen5 halamanHEAD NECK BACK SPINE SPECIAL TESTS December 2022Ted Lawrence CiscarBelum ada peringkat
- Knee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsDokumen36 halamanKnee Pain and Mobility Impairments: Meniscal and Articular Cartilage LesionsdedsnetBelum ada peringkat
- Introductio To OrthoticsDokumen8 halamanIntroductio To OrthoticsGopi Krishnan100% (1)
- Joint Range of Motion Assessment GuideDokumen16 halamanJoint Range of Motion Assessment GuideAlice Gifford100% (1)
- Arthrokinematics of Body Joints FinalDokumen3 halamanArthrokinematics of Body Joints FinalnmahpbooksBelum ada peringkat
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Barthel IndexDokumen2 halamanBarthel Indexgania100% (1)
- Beck Kognitiv Terapia Kezdőknek Es HaladoknakDokumen357 halamanBeck Kognitiv Terapia Kezdőknek Es HaladoknakÉva KappéterBelum ada peringkat
- RICHARD F. BAXTER-Pocket Guide To Musculoskeletal AssessmentDokumen104 halamanRICHARD F. BAXTER-Pocket Guide To Musculoskeletal Assessmentmaitre1959100% (4)
- Muscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)Dokumen177 halamanMuscle Stretching in Manual Therapy I - The Extremities (Team Nanban) (TPB)CNPOULIS100% (22)
- Dubrovnik enDokumen14 halamanDubrovnik enÉva KappéterBelum ada peringkat
- Manual in Single Doc-Dog Assisted TherapyDokumen268 halamanManual in Single Doc-Dog Assisted TherapyIoana Nechifor100% (1)
- Dynamics of Human GaitDokumen153 halamanDynamics of Human GaitKhalid100% (10)
- Fascial Manipulation Practical Part. ShleipDokumen72 halamanFascial Manipulation Practical Part. Shleiptrawn001100% (4)
- 044307402XPeripheralDokumen165 halaman044307402XPeripheralÉva Kappéter100% (1)
- Susan Edwards - Neurological PhysiotherapyDokumen293 halamanSusan Edwards - Neurological Physiotherapyharcaian_cristina90% (20)
- Anesthesia Options ExplainedDokumen6 halamanAnesthesia Options ExplainedSilvio DTBelum ada peringkat
- Medical Checkup ReportDokumen18 halamanMedical Checkup ReportFeliciaSetiawanBelum ada peringkat
- Abstract of Electrooculography Electrooculography (EOG) Is A New Technology of Placing Electrodes OnDokumen3 halamanAbstract of Electrooculography Electrooculography (EOG) Is A New Technology of Placing Electrodes OnFrancisco GomezBelum ada peringkat
- Identification of Species: VibrioDokumen13 halamanIdentification of Species: VibriomiluskaBelum ada peringkat
- XL22 - Basic HaematologyDokumen18 halamanXL22 - Basic HaematologyAdi TrisnoBelum ada peringkat
- A Components' Model of Addiction Within A Biopsychosocial FrameworkDokumen8 halamanA Components' Model of Addiction Within A Biopsychosocial FrameworkBognár ErzsébetBelum ada peringkat
- Children, Cell Phones, and Possible Side Effects Final DraftDokumen5 halamanChildren, Cell Phones, and Possible Side Effects Final DraftAngela Wentz-MccannBelum ada peringkat
- Useful Plants - Medicines: at LeastDokumen8 halamanUseful Plants - Medicines: at LeastJavier Yaguareté100% (1)
- Epidemiology Lectures by Dr. MabalatanDokumen8 halamanEpidemiology Lectures by Dr. MabalatanCitrusBelum ada peringkat
- Pulse OximetryDokumen38 halamanPulse OximetryJoanna Jauculan Albaño100% (2)
- Responsi HemoroidDokumen26 halamanResponsi HemoroidJessica Alexandria WuBelum ada peringkat
- Highly Skilled Medical Technologist Seeking New OpportunityDokumen8 halamanHighly Skilled Medical Technologist Seeking New Opportunityrosalyn cabucoBelum ada peringkat
- Dental Product CatalogDokumen193 halamanDental Product CatalogJeanBrinzaBelum ada peringkat
- Pharmacist 4Dokumen29 halamanPharmacist 4AHAMED SHIFAANBelum ada peringkat
- Rapid Rhino InstructionsDokumen2 halamanRapid Rhino InstructionsGolam SarwarBelum ada peringkat
- Nursing Exam Papers from Rajiv Gandhi UniversityDokumen10 halamanNursing Exam Papers from Rajiv Gandhi UniversityVantrigaru Veeresh Bangi100% (4)
- 2024-02-08 St. Mary's County TimesDokumen32 halaman2024-02-08 St. Mary's County TimesSouthern Maryland OnlineBelum ada peringkat
- Community DiagnosisDokumen28 halamanCommunity DiagnosisAlexious Marie CalluengBelum ada peringkat
- Three in A Row A Case Series of Cervical TuberculosisDokumen6 halamanThree in A Row A Case Series of Cervical TuberculosisJonelle baloloyBelum ada peringkat
- Verb Surgical - Surgery in The Digital AgeDokumen15 halamanVerb Surgical - Surgery in The Digital AgemedtechyBelum ada peringkat
- Moderate Sedation Consent Form: Authorization For The Administration of Conscious (Moderate) SedationDokumen1 halamanModerate Sedation Consent Form: Authorization For The Administration of Conscious (Moderate) SedationTribowo WicaksonoBelum ada peringkat
- Chapter 4 Drug MetabolismDokumen14 halamanChapter 4 Drug MetabolismNicole AguilarBelum ada peringkat
- KaoshikiiDokumen24 halamanKaoshikiiapi-238078813Belum ada peringkat
- Quantitative Analysis of Cordycepin in Cordyceps Militaris Under Different Extraction MethodsDokumen6 halamanQuantitative Analysis of Cordycepin in Cordyceps Militaris Under Different Extraction MethodsLượng Nguyễn VănBelum ada peringkat
- 05.03 - Interventional Neuroradiology PDFDokumen113 halaman05.03 - Interventional Neuroradiology PDFBivolaru AlinBelum ada peringkat
- Opinion WritingDokumen20 halamanOpinion WritingnirmalaBelum ada peringkat
- Code of EthicsDokumen10 halamanCode of Ethicsapi-316478139Belum ada peringkat
- Phimosis 5 PDFDokumen4 halamanPhimosis 5 PDFNurul YaqinBelum ada peringkat
- Mobile Games Addiction Corrupts OneDokumen1 halamanMobile Games Addiction Corrupts OnenanthiniBelum ada peringkat
- Updating The Definition of Pain.6Dokumen4 halamanUpdating The Definition of Pain.6Sesaria Fatimah Nur BahtiarBelum ada peringkat