Anda mungkin juga menyukai
- JAPS Review Article LatestDokumen5 halamanJAPS Review Article LatestSumit BediBelum ada peringkat
- JCM 08 00217 v3Dokumen23 halamanJCM 08 00217 v3Sumit BediBelum ada peringkat
- Antimicrobial Activity of Some Essential Oils-Present Status and Future Perspectives PDFDokumen21 halamanAntimicrobial Activity of Some Essential Oils-Present Status and Future Perspectives PDFTiền Kiếm100% (1)
- Super Monthly ChartsDokumen1 halamanSuper Monthly ChartsSumit BediBelum ada peringkat
- Virgo Horoscope Jan 2022Dokumen4 halamanVirgo Horoscope Jan 2022Sumit BediBelum ada peringkat
- Ijerph-18-11451 Meta Analysis StudyDokumen14 halamanIjerph-18-11451 Meta Analysis StudySumit BediBelum ada peringkat
- JAPS Journal For PublishingDokumen12 halamanJAPS Journal For PublishingSumit BediBelum ada peringkat
- Your February Horoscope For VirgoDokumen9 halamanYour February Horoscope For VirgoSumit BediBelum ada peringkat
- RJPT Instructions - To - AuthorDokumen2 halamanRJPT Instructions - To - AuthorSumit BediBelum ada peringkat
- 5 Essential OilsDokumen7 halaman5 Essential OilsSumit BediBelum ada peringkat
- Selected Investment Plays 2030Dokumen4 halamanSelected Investment Plays 2030Sumit BediBelum ada peringkat
- SELECTED INVESTMENT PLAYS 2030 (AutoRecovered)Dokumen3 halamanSELECTED INVESTMENT PLAYS 2030 (AutoRecovered)Sumit BediBelum ada peringkat
- Post Luting Goodacre PDFDokumen7 halamanPost Luting Goodacre PDFSumit BediBelum ada peringkat
- June Horoscope For VirgoDokumen6 halamanJune Horoscope For VirgoSumit BediBelum ada peringkat
- March Horoscope For Virgo 2022Dokumen4 halamanMarch Horoscope For Virgo 2022Sumit BediBelum ada peringkat
- Cariogram ManualDokumen51 halamanCariogram ManualJorge Velásquez100% (2)
- Ipo Strategy 2020-21 ListDokumen2 halamanIpo Strategy 2020-21 ListSumit BediBelum ada peringkat
- Jisppd PDFDokumen5 halamanJisppd PDFSumit BediBelum ada peringkat
- OSCE Based Assessment of Three Commonly Performed Pediatric Dentistry ProceduresDokumen6 halamanOSCE Based Assessment of Three Commonly Performed Pediatric Dentistry ProceduresSumit BediBelum ada peringkat
- Dental Licensure Step by Step IntlDokumen1 halamanDental Licensure Step by Step IntlSumit BediBelum ada peringkat
- Effects of Repeated Use On Bond Strengths of One-Bottle AdhesivesDokumen5 halamanEffects of Repeated Use On Bond Strengths of One-Bottle AdhesivesSumit BediBelum ada peringkat
- JISPPDDokumen5 halamanJISPPDSumit BediBelum ada peringkat
- How To Write A Successful Paper For The International Journal of Paediatric DentistryDokumen45 halamanHow To Write A Successful Paper For The International Journal of Paediatric DentistrySumit BediBelum ada peringkat
- Commonly Prescribed Medications in Pediatric Dentistry: Steven Schwartz, DDSDokumen25 halamanCommonly Prescribed Medications in Pediatric Dentistry: Steven Schwartz, DDSSumit BediBelum ada peringkat
- Stainless SteelDokumen6 halamanStainless SteelSumit BediBelum ada peringkat
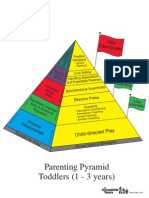
- Toddler Program PyramidDokumen1 halamanToddler Program Pyramidlutbas3379100% (1)
- Cavitypreparation 130320103634 Phpapp01Dokumen60 halamanCavitypreparation 130320103634 Phpapp01Sumit BediBelum ada peringkat
- Cavitypreparation 130320103634 Phpapp01Dokumen60 halamanCavitypreparation 130320103634 Phpapp01Sumit BediBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Armfield Et Al-2013-Australian Dental JournalDokumen18 halamanArmfield Et Al-2013-Australian Dental JournalAbhishek Isaac MathewBelum ada peringkat
- Ecde 18 01230Dokumen9 halamanEcde 18 01230Sudeep M. ChoudharyBelum ada peringkat
- AAPD Guideline on Behavior Guidance for Pediatric Dental PatientsDokumen9 halamanAAPD Guideline on Behavior Guidance for Pediatric Dental PatientsAzi Pertiwi HussainBelum ada peringkat
- EPQ Planning: Dental PhobiasDokumen7 halamanEPQ Planning: Dental PhobiasMatt246Belum ada peringkat
- Guideline On Behavior Guidance For The Pediatric Dental PatientDokumen14 halamanGuideline On Behavior Guidance For The Pediatric Dental Patientsabbath19Belum ada peringkat
- Dental Anxiety QuestionnairesDokumen4 halamanDental Anxiety QuestionnairesAmar BhochhibhoyaBelum ada peringkat
- Dental Pediatric Behavior GuidanceDokumen55 halamanDental Pediatric Behavior GuidanceAsala AbdulghaniBelum ada peringkat
- English Iii: University of Guayaquil Facultad Piloto de OdontologíaDokumen4 halamanEnglish Iii: University of Guayaquil Facultad Piloto de OdontologíaDianitaVelezPincayBelum ada peringkat
- Dental AnxietyDokumen3 halamanDental AnxietyLau Kien YeeBelum ada peringkat
- Parental Presence Vs Absence - Dr. Julie ManiateDokumen27 halamanParental Presence Vs Absence - Dr. Julie ManiateRooka82Belum ada peringkat
- List Of Phobias And Their Meanings ExplainedDokumen25 halamanList Of Phobias And Their Meanings ExplainedIdris Cia Sukubo100% (1)
- Managing Child in Dental Office by Non-Pharmacological Behavior Management TechniquesDokumen15 halamanManaging Child in Dental Office by Non-Pharmacological Behavior Management TechniquesIJAR JOURNALBelum ada peringkat
- AAPD BehavGuideDokumen18 halamanAAPD BehavGuideAhmad KhaledBelum ada peringkat
- BMC Oral HealthDokumen15 halamanBMC Oral HealthAlexandru Codrin-IonutBelum ada peringkat
- Patient ManagementDokumen101 halamanPatient ManagementRhutvi ViraniBelum ada peringkat
- Dental fear and anxiety in adult IcelandersDokumen5 halamanDental fear and anxiety in adult IcelandersSung Soon ChangBelum ada peringkat
- Translation and Validation of The Finnish Version of The Index of Dental Anxiety and Fear (IDAF-4C) Among Dental StudentsDokumen6 halamanTranslation and Validation of The Finnish Version of The Index of Dental Anxiety and Fear (IDAF-4C) Among Dental StudentsbaridinoBelum ada peringkat
- Behavior Guidance For The Pediatric Dental Patient: Latest RevisionDokumen19 halamanBehavior Guidance For The Pediatric Dental Patient: Latest RevisionJonathan Delgadillo VillarroelBelum ada peringkat
- Managing Dental Fear and AnxietyDokumen3 halamanManaging Dental Fear and AnxietySung Soon ChangBelum ada peringkat
- Dental Fear, Anxiety and Phobia (Final1)Dokumen55 halamanDental Fear, Anxiety and Phobia (Final1)Aj VishwadheebBelum ada peringkat
- Skala Prilaku FranklDokumen6 halamanSkala Prilaku FranklMeta Anjany FirmansyahBelum ada peringkat
- Age of Onset of Dental AnxietyDokumen7 halamanAge of Onset of Dental AnxietyHajar ChebliBelum ada peringkat
- Video modelling reduces dental anxiety in children receiving fissure sealantsDokumen5 halamanVideo modelling reduces dental anxiety in children receiving fissure sealantsfairuzBelum ada peringkat
- Sri Dwi Mutiara-Jurnal CRSS OSNE 1Dokumen11 halamanSri Dwi Mutiara-Jurnal CRSS OSNE 1sri dwi mutiaraBelum ada peringkat
- ODokumen11 halamanOMihaela CherejiBelum ada peringkat
- Berge - 2017 - Treatment of Intra Oral Injection Phobia A Randomized Delayed Intervention Controlled Trial Among Norwegian 10 To 16 Year OldsDokumen9 halamanBerge - 2017 - Treatment of Intra Oral Injection Phobia A Randomized Delayed Intervention Controlled Trial Among Norwegian 10 To 16 Year OldsEBelum ada peringkat
- Services Marketing Assignment 4Dokumen3 halamanServices Marketing Assignment 4Muhammad Osama AshrafBelum ada peringkat
- Dhyg 122 Dental Hygiene II Syllabus 2015Dokumen14 halamanDhyg 122 Dental Hygiene II Syllabus 2015api-284737097Belum ada peringkat
- Dental FearDokumen8 halamanDental FearShrishtiChokhaniBelum ada peringkat
- Journal 012010 PDFDokumen76 halamanJournal 012010 PDFAlysonBelum ada peringkat