Anda mungkin juga menyukai
- Internal Medicine NBME Form 3 ExplanationsDokumen11 halamanInternal Medicine NBME Form 3 ExplanationssasghfdgBelum ada peringkat
- POPS PretestDokumen6 halamanPOPS Pretestkingjameson1Belum ada peringkat
- Assessment Cover Sheet: Student To Complete Please Read The Below CarefullyDokumen25 halamanAssessment Cover Sheet: Student To Complete Please Read The Below CarefullyNoreen Punjwani100% (1)
- Medical Triads, Tetrads, and PentadsDokumen10 halamanMedical Triads, Tetrads, and PentadsAyessa BandalBelum ada peringkat
- Main Dip Step 2ck Notes Info Doc - Read OnlyDokumen305 halamanMain Dip Step 2ck Notes Info Doc - Read Only[161]Shuaib AktherBelum ada peringkat
- Medicine 1 Final Practical Exam ReviewerDokumen10 halamanMedicine 1 Final Practical Exam ReviewerTP RMadBelum ada peringkat
- Ethicon Wound Closure Manual - (February 2004)Dokumen127 halamanEthicon Wound Closure Manual - (February 2004)7052XX100% (1)
- Picot Research Paper - MullenDokumen16 halamanPicot Research Paper - Mullenapi-596714348Belum ada peringkat
- Incentive SpirometerDokumen25 halamanIncentive SpirometerAnalyn Salvacion100% (2)
- JI Chart OrdersDokumen4 halamanJI Chart OrdersMel BillonesBelum ada peringkat
- EndoDokumen8 halamanEndoSheryl Layne Lao-SebrioBelum ada peringkat
- Medicine Review 2018 1Dokumen470 halamanMedicine Review 2018 1Norjetalexis Maningo CabreraBelum ada peringkat
- B - Embyrology HomologuesDokumen1 halamanB - Embyrology HomologuesS ParekhBelum ada peringkat
- Amazing Esqs With Answers Pediatrics-ShelfDokumen31 halamanAmazing Esqs With Answers Pediatrics-ShelfDrSajid BuzdarBelum ada peringkat
- History Physical FormatDokumen3 halamanHistory Physical FormatfilchibuffBelum ada peringkat
- DeVirglio NotesDokumen77 halamanDeVirglio NotesAlvand SehatBelum ada peringkat
- Simplified Diagnostic Approach in Acute HepatitisDokumen2 halamanSimplified Diagnostic Approach in Acute HepatitisJohn Christopher LucesBelum ada peringkat
- Internal MedicineDokumen83 halamanInternal MedicineSumbul PBelum ada peringkat
- MED2 5.02 Oncologic Emergencies - Dr. F. AdefuinDokumen5 halamanMED2 5.02 Oncologic Emergencies - Dr. F. AdefuinAra DiocosBelum ada peringkat
- Neonatal Case Presentation 2Dokumen6 halamanNeonatal Case Presentation 2Rabi SyedBelum ada peringkat
- New Intern Guide Quick NotesDokumen8 halamanNew Intern Guide Quick NotesTrisBelum ada peringkat
- Correlative AnatomyDokumen19 halamanCorrelative AnatomyLicensed to HealBelum ada peringkat
- OSCE Reviewer 2013Dokumen4 halamanOSCE Reviewer 2013rere choiBelum ada peringkat
- Part IIDokumen64 halamanPart IIhussainBelum ada peringkat
- West Notes-1 PDFDokumen17 halamanWest Notes-1 PDFSerious LeoBelum ada peringkat
- Medicine OSCE - Common Diseases Ver2Dokumen4 halamanMedicine OSCE - Common Diseases Ver2TrisBelum ada peringkat
- Mo Intern Handbook - FinalDokumen37 halamanMo Intern Handbook - FinalGideon K. MutaiBelum ada peringkat
- Dem Tickler NotesDokumen1 halamanDem Tickler NotesSeff CausapinBelum ada peringkat
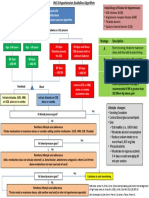
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDokumen1 halamanGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentMuthia ArsilBelum ada peringkat
- 22 Disritmia 2018Dokumen60 halaman22 Disritmia 2018Nur akilaBelum ada peringkat
- MTB Cardiology NotesDokumen11 halamanMTB Cardiology Noteskabal321Belum ada peringkat
- Aquifer InternalMedicine11 - 45Dokumen8 halamanAquifer InternalMedicine11 - 45JulieBelum ada peringkat
- 2011-09 - Ob-GynDokumen24 halaman2011-09 - Ob-Gynsahilius100% (1)
- Basic ECG For Refresher Course 2014Dokumen116 halamanBasic ECG For Refresher Course 2014Winz DolleteBelum ada peringkat
- GI Signs and SymptomsDokumen40 halamanGI Signs and SymptomsJohnny BeeBelum ada peringkat
- CPG DyslipidemiaDokumen26 halamanCPG DyslipidemiaRenzy SalumbreBelum ada peringkat
- 24 HR History 2Dokumen2 halaman24 HR History 2Arjun KatariaBelum ada peringkat
- Junior Intern NotesDokumen3 halamanJunior Intern NotesTin SumangaBelum ada peringkat
- JI RevalidaDokumen61 halamanJI RevalidaAren LingadBelum ada peringkat
- Mark Tuttle Neurology Clerkship Study Guide PDFDokumen84 halamanMark Tuttle Neurology Clerkship Study Guide PDFDavid ChangBelum ada peringkat
- Ob GynDokumen4 halamanOb Gynroserem2000Belum ada peringkat
- أدوية الطوارىءDokumen162 halamanأدوية الطوارىءManar22Belum ada peringkat
- SketchyPath ChecklistDokumen1 halamanSketchyPath ChecklistFajar Raza100% (1)
- HY Mixed USMLE Review Part I 1Dokumen20 halamanHY Mixed USMLE Review Part I 1Jennifer Ross-ComptisBelum ada peringkat
- Shock PresentationDokumen20 halamanShock Presentationrosalyn sugayBelum ada peringkat
- Clinical ExaminationDokumen11 halamanClinical ExaminationMavra zBelum ada peringkat
- GYNECOLOGY Chief ComplaintsDokumen3 halamanGYNECOLOGY Chief ComplaintsJennifer HerediaBelum ada peringkat
- USMLE Step 3 ER PDFDokumen12 halamanUSMLE Step 3 ER PDFlalaBelum ada peringkat
- Obstetric FormDokumen4 halamanObstetric FormKhylamarie VillalunaBelum ada peringkat
- IMDokumen128 halamanIMShaz ChindhyBelum ada peringkat
- Cheat Sheet (Draft)Dokumen3 halamanCheat Sheet (Draft)bonziebuddyBelum ada peringkat
- OB Med Order KodigsDokumen1 halamanOB Med Order KodigsfloramaeyecyecBelum ada peringkat
- IM NotesDokumen79 halamanIM NotesInri Dumlao100% (1)
- A Case of C.SDokumen85 halamanA Case of C.Sนีล ไบรอันBelum ada peringkat
- Poliomyelitis Haemophilus Influenzae Type B VariecellaDokumen4 halamanPoliomyelitis Haemophilus Influenzae Type B VariecellaJeanna Chong100% (1)
- 2020 Apr Common Treatment OrdersDokumen32 halaman2020 Apr Common Treatment OrdersAlistair LauBelum ada peringkat
- Aquifer InternalMedicine09 - 55Dokumen7 halamanAquifer InternalMedicine09 - 55JulieBelum ada peringkat
- Neonatology I: Pediatrics 1.1Dokumen15 halamanNeonatology I: Pediatrics 1.1Kurt ZepedaBelum ada peringkat
- Fabella NotesDokumen96 halamanFabella NotesAndrassy Twinkle AlineaBelum ada peringkat
- Pedia HXDokumen3 halamanPedia HXeyakoyBelum ada peringkat
- Problem-based Approach to Gastroenterology and HepatologyDari EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisBelum ada peringkat
- Catheterisation OSCE Mark SchemeDokumen2 halamanCatheterisation OSCE Mark Schememyat252Belum ada peringkat
- AnovaDokumen80 halamanAnovamyat252Belum ada peringkat
- Ampullary CADokumen11 halamanAmpullary CAmyat252Belum ada peringkat
- Gallbladdercancer: Diagnosis, Surgical Management, and Adjuvant TherapiesDokumen19 halamanGallbladdercancer: Diagnosis, Surgical Management, and Adjuvant Therapiesmyat252Belum ada peringkat
- Asa Physical Status Classification SystemDokumen1 halamanAsa Physical Status Classification Systemmyat252Belum ada peringkat
- NG InsertionDokumen3 halamanNG Insertionmyat252Belum ada peringkat
- Example of Bad Answer: Press The Number of The Question To Get The AnswerDokumen12 halamanExample of Bad Answer: Press The Number of The Question To Get The Answermyat252Belum ada peringkat
- Anaemia - B12 and Folate Deficiency: SummaryDokumen16 halamanAnaemia - B12 and Folate Deficiency: Summarymyat252100% (1)
- Benko Gambit Move by MoveDokumen189 halamanBenko Gambit Move by Movemyat25290% (10)
- Samsung Galaxy Tab s4 MANUALDokumen159 halamanSamsung Galaxy Tab s4 MANUALmyat252Belum ada peringkat
- Ent Notes Moammed AteegDokumen39 halamanEnt Notes Moammed Ateegmyat252Belum ada peringkat
- CAPD PeritonitisDokumen1 halamanCAPD Peritonitismyat252Belum ada peringkat
- Nervous SystemDokumen62 halamanNervous Systemmyat252Belum ada peringkat
- Duplex Scan Kidneys: Abdo USSDokumen1 halamanDuplex Scan Kidneys: Abdo USSmyat252Belum ada peringkat
- NICE SummariesDokumen21 halamanNICE Summariesmyat252Belum ada peringkat
- Acinetobacter PDFDokumen1 halamanAcinetobacter PDFmyat252Belum ada peringkat
- Bone Marrow Transplant - Pulmonary ComplicationsDokumen1 halamanBone Marrow Transplant - Pulmonary Complicationsmyat252Belum ada peringkat
- Adjunctive Respiratory TherapiesDokumen1 halamanAdjunctive Respiratory Therapiesmyat252Belum ada peringkat
- Chronic Disease MXDokumen263 halamanChronic Disease MXmyat252Belum ada peringkat
- Opthamology AKT Study This Set Online atDokumen6 halamanOpthamology AKT Study This Set Online atmyat252Belum ada peringkat
- Surgery FinalADokumen102 halamanSurgery FinalAvaegmundig100% (1)
- Surgery Shock PDFDokumen9 halamanSurgery Shock PDFmyat252Belum ada peringkat
- CSA ABC 50 Top Tips To Pass The CSADokumen25 halamanCSA ABC 50 Top Tips To Pass The CSAmyat252Belum ada peringkat
- SurgeryDokumen48 halamanSurgerymyat252Belum ada peringkat
- Oncology AKT Study This Set Online atDokumen1 halamanOncology AKT Study This Set Online atmyat252Belum ada peringkat
- MeningitisDokumen2 halamanMeningitismyat252Belum ada peringkat
- Complete MRCGP Revision GuideDokumen45 halamanComplete MRCGP Revision Guidemyat2520% (3)
- Fauci Dossier Valentine S Day Document 2022 (1) SummaryDokumen5 halamanFauci Dossier Valentine S Day Document 2022 (1) SummarySherri StreightBelum ada peringkat
- Beta 2 AgonistsDokumen198 halamanBeta 2 AgonistsLeonardo FerreiraBelum ada peringkat
- Using A Dense PTFE Membrane Without Primary Closure To Achieve Bone and Tissue RegenerationDokumen5 halamanUsing A Dense PTFE Membrane Without Primary Closure To Achieve Bone and Tissue RegenerationDiego SiqueiraBelum ada peringkat
- Biosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustDokumen25 halamanBiosafety and Bioethics of Biotechnology ABS-832: DR Attya Bhatti Assistant Professor Head of Department Asab-NustAviation MedicineBelum ada peringkat
- Mikrobiologi DiagramDokumen2 halamanMikrobiologi Diagrampuguh89Belum ada peringkat
- Tipos de SuturasDokumen5 halamanTipos de SuturasLeandro PeraltaBelum ada peringkat
- Integrated Vector Control ProgramDokumen35 halamanIntegrated Vector Control ProgramKeerthi VasanBelum ada peringkat
- Local AnestheticDokumen4 halamanLocal AnestheticAndrea TrescotBelum ada peringkat
- HR Policy ManualDokumen34 halamanHR Policy Manualshamna AbdullaBelum ada peringkat
- Oxygen Therapy For NurseDokumen46 halamanOxygen Therapy For NurseselviiBelum ada peringkat
- Fracture of The Upper HumerusDokumen22 halamanFracture of The Upper HumerusOlasinde AnthonyBelum ada peringkat
- Supervisor: Prof. Dr. Atan Baas Sinuhaji, Spa (K)Dokumen35 halamanSupervisor: Prof. Dr. Atan Baas Sinuhaji, Spa (K)Ranap HadiyantoBelum ada peringkat
- Five"EFFICACY OF GANDHARVAHASTADI KASHAYAM IN THE MANAGEMENT OF ESSENTIAL HYPERTENSION (UCCHA - RAKTHACHAAPA)Dokumen12 halamanFive"EFFICACY OF GANDHARVAHASTADI KASHAYAM IN THE MANAGEMENT OF ESSENTIAL HYPERTENSION (UCCHA - RAKTHACHAAPA)Pradeep SambandamBelum ada peringkat
- Tosoh Series 2147Dokumen3 halamanTosoh Series 2147ShahinBelum ada peringkat
- Tanda, Ciri-Ciri Dan Perbedaan Versi B InggrisDokumen2 halamanTanda, Ciri-Ciri Dan Perbedaan Versi B Inggriselama natilaBelum ada peringkat
- Radioembolization of Hepatic Malignancies - Background, Quality Improvement Guidelines, and Future DirectionsDokumen15 halamanRadioembolization of Hepatic Malignancies - Background, Quality Improvement Guidelines, and Future DirectionsVeronica AlexanderBelum ada peringkat
- Lesson Plan BrochodilatorsDokumen14 halamanLesson Plan BrochodilatorsVaishali SinghBelum ada peringkat
- ELISIO Clinical StudiesDokumen12 halamanELISIO Clinical StudiesIndra NugrohoBelum ada peringkat
- Chylothorax OriginalDokumen4 halamanChylothorax OriginalMaria CostandachiBelum ada peringkat
- Franco, Danica A. (Cardio)Dokumen5 halamanFranco, Danica A. (Cardio)Danica FrancoBelum ada peringkat
- Endocrine DisordersDokumen106 halamanEndocrine DisordersMansur MuhammadBelum ada peringkat
- Silicone - MSDS - PT. Lemindo IndonesiaDokumen6 halamanSilicone - MSDS - PT. Lemindo IndonesialiemsaputrarendiBelum ada peringkat
- 2 AleDokumen10 halaman2 AleAna María ReyesBelum ada peringkat
- The Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic DiseaseDokumen14 halamanThe Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic DiseaseVenny SarumpaetBelum ada peringkat
- Lecture Notes On AphDokumen41 halamanLecture Notes On AphEyob MizanBelum ada peringkat
- Cardiovascular Examination: Preparation of The PatientDokumen4 halamanCardiovascular Examination: Preparation of The PatientLolla SinwarBelum ada peringkat