Anda mungkin juga menyukai
- CPR in Term Pregnancies-19Dokumen23 halamanCPR in Term Pregnancies-19Blanca Herrera MoralesBelum ada peringkat
- Cardiomiopatia Inducida Por StressDokumen8 halamanCardiomiopatia Inducida Por StressBlanca Herrera MoralesBelum ada peringkat
- Cardiomiopatia Hipertrofica 2016 PDFDokumen25 halamanCardiomiopatia Hipertrofica 2016 PDFBlanca Herrera MoralesBelum ada peringkat
- Extracardiac Signs of Fluid Overload in The Critically IllDokumen13 halamanExtracardiac Signs of Fluid Overload in The Critically IllBlanca Herrera MoralesBelum ada peringkat
- Medical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesDokumen20 halamanMedical Clinics of North America Volume 101 Issue 3 2017 (Doi 10.1016 - J.mcna.2016.12.011) Fayfman, Maya Pasquel, Francisco J. Umpierrez, Guillermo E. - Management of Hyperglycemic CrisesBlanca Herrera MoralesBelum ada peringkat
- Prediction of Fluid Responsiveness An Up DateDokumen11 halamanPrediction of Fluid Responsiveness An Up DateBlanca Herrera MoralesBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
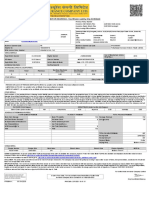
- MOTOR INSURANCE - Two Wheeler Liability Only SCHEDULEDokumen1 halamanMOTOR INSURANCE - Two Wheeler Liability Only SCHEDULESuhail V VBelum ada peringkat
- Unit 2Dokumen97 halamanUnit 2MOHAN RuttalaBelum ada peringkat
- Ikea AnalysisDokumen33 halamanIkea AnalysisVinod BridglalsinghBelum ada peringkat
- A320 TakeoffDokumen17 halamanA320 Takeoffpp100% (1)
- HSBC in A Nut ShellDokumen190 halamanHSBC in A Nut Shelllanpham19842003Belum ada peringkat
- Health Insurance in Switzerland ETHDokumen57 halamanHealth Insurance in Switzerland ETHguzman87Belum ada peringkat
- BluetoothDokumen28 halamanBluetoothMilind GoratelaBelum ada peringkat
- Topic 4: Mental AccountingDokumen13 halamanTopic 4: Mental AccountingHimanshi AryaBelum ada peringkat
- Escario Vs NLRCDokumen10 halamanEscario Vs NLRCnat_wmsu2010Belum ada peringkat
- Squirrel Cage Induction Motor Preventive MaintenaceDokumen6 halamanSquirrel Cage Induction Motor Preventive MaintenaceNishantPareekBelum ada peringkat
- Digital LiteracyDokumen19 halamanDigital Literacynagasms100% (1)
- T1500Z / T2500Z: Coated Cermet Grades With Brilliant Coat For Steel TurningDokumen16 halamanT1500Z / T2500Z: Coated Cermet Grades With Brilliant Coat For Steel TurninghosseinBelum ada peringkat
- FIRE FIGHTING ROBOT (Mini Project)Dokumen21 halamanFIRE FIGHTING ROBOT (Mini Project)Hisham Kunjumuhammed100% (2)
- Hotel Reservation SystemDokumen36 halamanHotel Reservation SystemSowmi DaaluBelum ada peringkat
- General Financial RulesDokumen9 halamanGeneral Financial RulesmskBelum ada peringkat
- Privacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryDokumen50 halamanPrivacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryAbid KhanBelum ada peringkat
- Government of West Bengal Finance (Audit) Department: NABANNA', HOWRAH-711102 No. Dated, The 13 May, 2020Dokumen2 halamanGovernment of West Bengal Finance (Audit) Department: NABANNA', HOWRAH-711102 No. Dated, The 13 May, 2020Satyaki Prasad MaitiBelum ada peringkat
- Information Security Chapter 1Dokumen44 halamanInformation Security Chapter 1bscitsemvBelum ada peringkat
- Continue: Rudolf Bultmann Theology of The New Testament PDFDokumen3 halamanContinue: Rudolf Bultmann Theology of The New Testament PDFpishoi gerges0% (1)
- Schmidt Family Sales Flyer English HighDokumen6 halamanSchmidt Family Sales Flyer English HighmdeenkBelum ada peringkat
- 09 WA500-3 Shop ManualDokumen1.335 halaman09 WA500-3 Shop ManualCristhian Gutierrez Tamayo93% (14)
- Introduce Letter - CV IDS (Company Profile)Dokumen13 halamanIntroduce Letter - CV IDS (Company Profile)katnissBelum ada peringkat
- Innovations in Land AdministrationDokumen66 halamanInnovations in Land AdministrationSanjawe KbBelum ada peringkat
- CANELA Learning Activity - NSPE Code of EthicsDokumen4 halamanCANELA Learning Activity - NSPE Code of EthicsChristian CanelaBelum ada peringkat
- CoDokumen80 halamanCogdayanand4uBelum ada peringkat
- 18PGHR11 - MDI - Aditya JainDokumen4 halaman18PGHR11 - MDI - Aditya JainSamanway BhowmikBelum ada peringkat
- Unit-5 Shell ProgrammingDokumen11 halamanUnit-5 Shell ProgrammingLinda BrownBelum ada peringkat
- Shubham RBSEDokumen13 halamanShubham RBSEShubham Singh RathoreBelum ada peringkat
- Dissertation On Indian Constitutional LawDokumen6 halamanDissertation On Indian Constitutional LawCustomPaperWritingAnnArbor100% (1)
- MSDS - Tuff-Krete HD - Part DDokumen6 halamanMSDS - Tuff-Krete HD - Part DAl GuinitaranBelum ada peringkat