Anda mungkin juga menyukai
- Breath Sounds Incredibly EasyDokumen4 halamanBreath Sounds Incredibly EasyMatthew Ryan100% (3)
- Respiratory System-Review PathoDokumen100 halamanRespiratory System-Review PathoSadiePartington-RiopelleBelum ada peringkat
- Patho Cheat SheetDokumen18 halamanPatho Cheat SheetJaney T.Belum ada peringkat
- Respiratory SystemDokumen36 halamanRespiratory SystemPritha Bhuwapaksophon100% (1)
- Physiology of Phonation: Laryngeal Function and Vocal RegistersDokumen10 halamanPhysiology of Phonation: Laryngeal Function and Vocal RegistersDeane BiancaBelum ada peringkat
- Breath Sounds: ConsiderationsDokumen10 halamanBreath Sounds: ConsiderationsKarl RobleBelum ada peringkat
- Industry Perspective On Medical Risk of Visible Particles in Injectable ProductsDokumen22 halamanIndustry Perspective On Medical Risk of Visible Particles in Injectable Productsdavincicode888Belum ada peringkat
- Patient with fever: Causes and typesDokumen46 halamanPatient with fever: Causes and typesNosheen hafeez100% (1)
- A Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- General MCQDokumen43 halamanGeneral MCQalh basharBelum ada peringkat
- Sarcoidosis DR WinnieDokumen33 halamanSarcoidosis DR WinniewinnieBelum ada peringkat
- A Pattern Approach To Lymph Node Diagnosis - A. Leong (Springer, 2011) WWDokumen432 halamanA Pattern Approach To Lymph Node Diagnosis - A. Leong (Springer, 2011) WWAdrian TirlaBelum ada peringkat
- RespiratoryDokumen34 halamanRespiratoryanasokour100% (1)
- Auscultation of The Respiratory SystemDokumen30 halamanAuscultation of The Respiratory SystemRodriBelum ada peringkat
- Lung Auscultation Sounds GuideDokumen3 halamanLung Auscultation Sounds GuideCristina TofanBelum ada peringkat
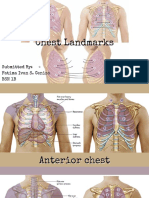
- Thorax and Lungs ReferenceDokumen8 halamanThorax and Lungs Referencegwynth ripaldaBelum ada peringkat
- Lung Sounds Guide: Vesicular, Bronchial, Crackles & MoreDokumen24 halamanLung Sounds Guide: Vesicular, Bronchial, Crackles & MoreAswinBelum ada peringkat
- Breath SoundDokumen4 halamanBreath SoundkamaluBelum ada peringkat
- Lung AuscultationDokumen62 halamanLung AuscultationOlea CroitorBelum ada peringkat
- The Breath Sounds: Intensity (Or Loudness)Dokumen6 halamanThe Breath Sounds: Intensity (Or Loudness)Santhosh KumarBelum ada peringkat
- Types of Breath SoundDokumen2 halamanTypes of Breath SoundArslan HassanBelum ada peringkat
- IPPADokumen4 halamanIPPAIsaac KipchumbaBelum ada peringkat
- Examination of The Chest (Auscultation)Dokumen21 halamanExamination of The Chest (Auscultation)Mahmoud AbouelsoudBelum ada peringkat
- Pemahaman Suara NapasDokumen21 halamanPemahaman Suara NapashengkiBelum ada peringkat
- Lung Examination: AbnormalDokumen56 halamanLung Examination: AbnormalBECAREFUL89ABelum ada peringkat
- 3 en AusculationDokumen22 halaman3 en AusculationsajidmuBelum ada peringkat
- Auscultation of the Lungs: A Guide to Lung Sound AssessmentDokumen11 halamanAuscultation of the Lungs: A Guide to Lung Sound AssessmentFamilia Macovei Haralambie-AndreeaBelum ada peringkat
- Cardio AssessementDokumen9 halamanCardio AssessementPoonam soniBelum ada peringkat
- Topic 8 Resp SystDokumen16 halamanTopic 8 Resp SystIlaaBelum ada peringkat
- Suara ParuDokumen31 halamanSuara ParuSuyanto nduduBelum ada peringkat
- Understanding Airstream MechanismsDokumen5 halamanUnderstanding Airstream MechanismsZena SattarBelum ada peringkat
- Lung SoundDokumen2 halamanLung SoundRJay AlavazoBelum ada peringkat
- Auscultation Sites and Normal Breath SoundsDokumen22 halamanAuscultation Sites and Normal Breath SoundsFatima Ivan CenizaBelum ada peringkat
- Terms chronic bronchitis Hemoptysis definitionsDokumen5 halamanTerms chronic bronchitis Hemoptysis definitionsDiane Kate Tobias MagnoBelum ada peringkat
- Name: Jake Yvan G. Dizon Year Level: BSN IIIDokumen2 halamanName: Jake Yvan G. Dizon Year Level: BSN IIIJake Yvan DizonBelum ada peringkat
- MVS Pulmonary AuscultationDokumen8 halamanMVS Pulmonary Auscultationvashini9151Belum ada peringkat
- Physiology of LarynxDokumen13 halamanPhysiology of LarynxsallykamareddineBelum ada peringkat
- Oxygenation 1Dokumen155 halamanOxygenation 1Khatlen BagaresBelum ada peringkat
- Lung Sounds Auscultation - 1Dokumen3 halamanLung Sounds Auscultation - 1George BarajazBelum ada peringkat
- NEJM 2014 Fundamentals of Lung AuscultationDokumen7 halamanNEJM 2014 Fundamentals of Lung AuscultationFelipe CeaBelum ada peringkat
- Rev Widya Physical Examination of Respiratory SystemDokumen72 halamanRev Widya Physical Examination of Respiratory SystemYuliaBelum ada peringkat
- Pulmonary Examination - Knowledge at AMBOSSDokumen1 halamanPulmonary Examination - Knowledge at AMBOSSKC Dela RosaBelum ada peringkat
- Pulmonary Ventilation: Dr. Mohamed HassanDokumen29 halamanPulmonary Ventilation: Dr. Mohamed HassanSAKARIYE MAXAMEDBelum ada peringkat
- CracklesDokumen6 halamanCracklesFernando Sánchez DíezBelum ada peringkat
- Chapter 40. Nursing Care of A Child With Respiratory Disorder TermsDokumen3 halamanChapter 40. Nursing Care of A Child With Respiratory Disorder TermsJœnríčk AzueloBelum ada peringkat
- 1.) Anatomy and Physiology of The Respiratory SystemDokumen6 halaman1.) Anatomy and Physiology of The Respiratory SystemFaith SarmientoBelum ada peringkat
- Lung Sounds: Inasa Nabila 1810211113Dokumen10 halamanLung Sounds: Inasa Nabila 1810211113Inasa NabilaBelum ada peringkat
- Lung Sounds On Percussion and AuscultationDokumen3 halamanLung Sounds On Percussion and AuscultationKanika GuptaBelum ada peringkat
- Respiratory SystemDokumen43 halamanRespiratory SystemAbuhuraira RafiqBelum ada peringkat
- 10.2. Respiratory Examination -邓旺Dokumen89 halaman10.2. Respiratory Examination -邓旺mirabel IvanaliBelum ada peringkat
- Roses Are Red, Violets Are Blue, Without Your Lungs Your Blood Would Be, Too.Dokumen249 halamanRoses Are Red, Violets Are Blue, Without Your Lungs Your Blood Would Be, Too.MabesBelum ada peringkat
- Thorax ExaminationDokumen3 halamanThorax Examinationyulis setiawatiBelum ada peringkat
- Adventitious Breath Sounds - HandoutDokumen2 halamanAdventitious Breath Sounds - Handoutkaren solibaBelum ada peringkat
- Respiratory SystemDokumen7 halamanRespiratory SystemxoxogeloBelum ada peringkat
- Abnormal Breath SoundsDokumen3 halamanAbnormal Breath SoundsIndra PermanaBelum ada peringkat
- Respiratory SoundsDokumen2 halamanRespiratory SoundsMuhammad NaeemjakBelum ada peringkat
- CP4. Respiratory SystemDokumen28 halamanCP4. Respiratory Systemdafabc50Belum ada peringkat
- Clinical Significance of Breath Sounds in Respiratory AssessmentDokumen16 halamanClinical Significance of Breath Sounds in Respiratory AssessmentWamique IzharBelum ada peringkat
- Anatomi Dan Fisiologi Jalan NafasDokumen54 halamanAnatomi Dan Fisiologi Jalan NafasFajhriaLeeBelum ada peringkat
- Respiratory PhysiologyDokumen9 halamanRespiratory PhysiologyBrent TorresBelum ada peringkat
- Pemeriksaan ThoraxDokumen27 halamanPemeriksaan ThoraxYaasinta ArlaesBelum ada peringkat
- Lung ExaminationDokumen14 halamanLung Examinationსალომე მუმლაძე “Slay” TMABelum ada peringkat
- Sailor Hospitalized with HemoptysisDokumen18 halamanSailor Hospitalized with HemoptysisMarissaevisBelum ada peringkat
- Encyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Dari EverandEncyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Belum ada peringkat
- Encyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Dari EverandEncyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Belum ada peringkat
- Caso 1Dokumen14 halamanCaso 1Luanna DávilaBelum ada peringkat
- Second Class UveitisDokumen42 halamanSecond Class Uveitisabhishek tBelum ada peringkat
- Pathology 2 TND LiveDokumen38 halamanPathology 2 TND Livepavan kumarBelum ada peringkat
- Tuberculosis Diagnosis and TreatmentDokumen46 halamanTuberculosis Diagnosis and TreatmentMoses Jr KazevuBelum ada peringkat
- Ear Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniDokumen76 halamanEar Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniAldy Bima100% (1)
- Diseases of TunasDokumen20 halamanDiseases of Tunasginger1984Belum ada peringkat
- Feline Infectious Peritonitis Pada Kucing LokalDokumen10 halamanFeline Infectious Peritonitis Pada Kucing Lokalandi nur indriBelum ada peringkat
- Acute & Chronic InflammationDokumen24 halamanAcute & Chronic Inflammationapi-19916399Belum ada peringkat
- VasculittisDokumen28 halamanVasculittisBernamai CalamBelum ada peringkat
- Inflammation and HealingDokumen30 halamanInflammation and HealingKoustubh JoshiBelum ada peringkat
- Dentosphere - World of Dentistry - MCQs On Pulp and Periapical PathologyDokumen8 halamanDentosphere - World of Dentistry - MCQs On Pulp and Periapical PathologyHadeel AltelbanyBelum ada peringkat
- Escleritis Necrotizante 3casosDokumen5 halamanEscleritis Necrotizante 3casosMario Cesar Islas SánchezBelum ada peringkat
- Peripheral LymphadenopathyDokumen11 halamanPeripheral LymphadenopathyserubimBelum ada peringkat
- VasculitisDokumen63 halamanVasculitisPutu 'yayuk' Widyani WiradiraniBelum ada peringkat
- Pathology Lec 7Dokumen63 halamanPathology Lec 7ahmadBelum ada peringkat
- Pulmonary Heart DiseaseDokumen379 halamanPulmonary Heart DiseaseJose CastellonBelum ada peringkat
- What causes leprosy and its symptomsDokumen7 halamanWhat causes leprosy and its symptomsArron Buenavista AblogBelum ada peringkat
- Pathology ProtocolsDokumen33 halamanPathology ProtocolsLin AdutBelum ada peringkat
- Histopathology Chapter 1Dokumen92 halamanHistopathology Chapter 1Zelalem DejazmachBelum ada peringkat
- Patologi MataDokumen30 halamanPatologi Matasiti agusriantinaBelum ada peringkat
- 01 FNAC Approach To Scrotal MassesDokumen3 halaman01 FNAC Approach To Scrotal MassescandiddreamsBelum ada peringkat
- Why Does My Patient Limphadenopathy or Splenomegaly?Dokumen14 halamanWhy Does My Patient Limphadenopathy or Splenomegaly?lacmftcBelum ada peringkat
- Basic Skin Histopathology: Dr. Najeeb Ullah Khan Trainee Fcps Dermatology KTH PeshawarDokumen82 halamanBasic Skin Histopathology: Dr. Najeeb Ullah Khan Trainee Fcps Dermatology KTH PeshawarJohn100% (1)
- 11 Lung PathologyDokumen7 halaman11 Lung PathologycarlgangcaBelum ada peringkat