Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Nidhi ResumeDokumen2 halamanNidhi ResumeabhiBelum ada peringkat
- G3412 - 450 KW Performance DataDokumen3 halamanG3412 - 450 KW Performance DataJacob De CasillasBelum ada peringkat
- Grade 10 CH 6 Assertion Reason QuestionsDokumen5 halamanGrade 10 CH 6 Assertion Reason QuestionsVidhun 8ABelum ada peringkat
- 新型重油催化裂化催化剂RCC 1的研究开发Dokumen5 halaman新型重油催化裂化催化剂RCC 1的研究开发Anca DumitruBelum ada peringkat
- Vensim User ManualDokumen34 halamanVensim User ManualMahdan LondoBelum ada peringkat
- Ra 6938Dokumen2 halamanRa 6938GaryBelum ada peringkat
- Hazardous Area ClassificationDokumen36 halamanHazardous Area Classificationvenkeeku100% (1)
- Strain STREMADokumen6 halamanStrain STREMAChavin StormBelum ada peringkat
- Mit BBM (Ib), Ipm-Session 2.4Dokumen32 halamanMit BBM (Ib), Ipm-Session 2.4Yogesh AdhateBelum ada peringkat
- Ruby On Rails 3 Cheat SheetDokumen7 halamanRuby On Rails 3 Cheat SheetJarosław MedwidBelum ada peringkat
- Frequency AdverbsDokumen4 halamanFrequency AdverbsAlexander ScrBelum ada peringkat
- Ee-502 Unit - IDokumen2 halamanEe-502 Unit - IVARAPRASADBelum ada peringkat
- Optical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andDokumen19 halamanOptical Properties of Gem Substances Educational Objective: This Exercise, Unit 7 in The Above Syllabus, Will Introduce Students To Skills andCarl SoriaBelum ada peringkat
- D4304-Syllabus-Neural Networks and Fuzzy SystemsDokumen1 halamanD4304-Syllabus-Neural Networks and Fuzzy Systemsshankar15050% (1)
- Form in MusicDokumen8 halamanForm in MusicAndri KurniawanBelum ada peringkat
- Helmholtz Resonance - Wikipedia, The Free EncyclopediaDokumen4 halamanHelmholtz Resonance - Wikipedia, The Free Encyclopediahamidah1963Belum ada peringkat
- Binary PDFDokumen13 halamanBinary PDFbyprasadBelum ada peringkat
- Data Download CMM366A-4G V1.0 enDokumen16 halamanData Download CMM366A-4G V1.0 enSuramanBelum ada peringkat
- Elementary Surveying Problem Set 2 q1Dokumen2 halamanElementary Surveying Problem Set 2 q1soontobengineer50% (2)
- Math Formula SheetDokumen8 halamanMath Formula SheetHidayah TeacherBelum ada peringkat
- C V RamanDokumen8 halamanC V RamanJayesh KomalwarBelum ada peringkat
- B 1 1 4 Inplant Fluid FlowDokumen5 halamanB 1 1 4 Inplant Fluid FlowBolívar AmoresBelum ada peringkat
- Hiley TableDokumen5 halamanHiley TableHanafiahHamzahBelum ada peringkat
- The Power of Adventure in Your Hand: Product Catalog Volume 4 2019Dokumen20 halamanThe Power of Adventure in Your Hand: Product Catalog Volume 4 2019Michael ShelbyBelum ada peringkat
- DS1103 Datasheet PDFDokumen6 halamanDS1103 Datasheet PDFRosario RiveraBelum ada peringkat
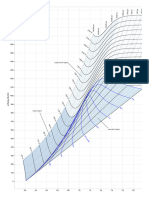
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDokumen1 halamanMollier Enthalpy Entropy Chart For Steam - US Unitslin tongBelum ada peringkat
- Script Track IP TermuxDokumen5 halamanScript Track IP TermuxAsepBelum ada peringkat
- JSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogDokumen7 halamanJSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogMartin MurciegoBelum ada peringkat
- Numerical ModelDokumen61 halamanNumerical ModelAlbert AguileraBelum ada peringkat
- DLP Mathematics 6 q1 w6Dokumen5 halamanDLP Mathematics 6 q1 w6Kathlyn PerezBelum ada peringkat