Anda mungkin juga menyukai
- Estudio 2ladyDokumen9 halamanEstudio 2ladymauricio ocampoBelum ada peringkat
- Nejmoa 1904340Dokumen11 halamanNejmoa 1904340LUIS ALFREDO SALGADO FLORESBelum ada peringkat
- 10 1093@jac@dky192Dokumen8 halaman10 1093@jac@dky192Rahmad SyamsulBelum ada peringkat
- LENACAPAVIRDokumen11 halamanLENACAPAVIRAhmed ElgenaidyBelum ada peringkat
- The Safety Effectiveness and ConcentratiDokumen5 halamanThe Safety Effectiveness and ConcentratiOtaku MasterBelum ada peringkat
- Deber #2 Medicina TropicalDokumen7 halamanDeber #2 Medicina TropicalGabriel Ernesto OlveraBelum ada peringkat
- Recent Advances in Antiviral Therapy: Derek KinchingtonDokumen7 halamanRecent Advances in Antiviral Therapy: Derek KinchingtonYogesh RathiBelum ada peringkat
- High-Dose Ceftriaxone Safety in CNS InfectionsDokumen8 halamanHigh-Dose Ceftriaxone Safety in CNS InfectionsRinaldy TejaBelum ada peringkat
- DTG VS RTGDokumen9 halamanDTG VS RTGThanawan TippayamongkolkulBelum ada peringkat
- Luo 2019 - Incidence and Types of HIV-1 Drug Resistance Mutation Among Patients Failing First-Line Antiretroviral TherapyDokumen5 halamanLuo 2019 - Incidence and Types of HIV-1 Drug Resistance Mutation Among Patients Failing First-Line Antiretroviral TherapyAndrew BanksBelum ada peringkat
- TMP 8 FA6Dokumen6 halamanTMP 8 FA6FrontiersBelum ada peringkat
- Articles: BackgroundDokumen9 halamanArticles: BackgroundSheroline BackBelum ada peringkat
- Molnupiravir EVIDoa2100044Dokumen13 halamanMolnupiravir EVIDoa2100044Doug StevensBelum ada peringkat
- 31 5 1155Dokumen9 halaman31 5 1155operation_cloudburstBelum ada peringkat
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDokumen10 halamanSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionSitta Grewo LiandarBelum ada peringkat
- Mathur 2015Dokumen7 halamanMathur 2015Maximiliano OliveraBelum ada peringkat
- EDEN UNIVERSITY HEALTH SCIENCES ASSIGNMENTDokumen25 halamanEDEN UNIVERSITY HEALTH SCIENCES ASSIGNMENTJoseph A MwitupaBelum ada peringkat
- Bedaquiline Article Multidrug-Resistant TuberculosisDokumen10 halamanBedaquiline Article Multidrug-Resistant TuberculosisAlvaro MuñozBelum ada peringkat
- Scorpion Envenomation and Serotherapy inDokumen7 halamanScorpion Envenomation and Serotherapy inrijal fahrijalBelum ada peringkat
- ElalfyEtal210213 TrmtCovid-IVM+Zn+Ribavirin+NitazoxanideDokumen8 halamanElalfyEtal210213 TrmtCovid-IVM+Zn+Ribavirin+NitazoxanideR NobleBelum ada peringkat
- Full TextDokumen12 halamanFull TextmagnodsgBelum ada peringkat
- Antimicrobial Agents and Chemotherapy-2009-Svetitsky-4069.fullDokumen11 halamanAntimicrobial Agents and Chemotherapy-2009-Svetitsky-4069.fullanuj singhBelum ada peringkat
- Dooley 2020Dokumen9 halamanDooley 2020wahyuni yuniBelum ada peringkat
- Nejmoa 1310480Dokumen11 halamanNejmoa 1310480mz zumrodinBelum ada peringkat
- Meningitis 3Dokumen12 halamanMeningitis 3Kelly MuñozBelum ada peringkat
- Baxter 2020Dokumen12 halamanBaxter 2020yalocim666Belum ada peringkat
- Combination DrugsDokumen16 halamanCombination DrugsValerie Gonzaga-CarandangBelum ada peringkat
- Fase 1.2Dokumen11 halamanFase 1.2Verliatesya TugasBelum ada peringkat
- Babesiosis As A Rare Cause of Fever in The Immunocompromised Patient: A Case ReportDokumen5 halamanBabesiosis As A Rare Cause of Fever in The Immunocompromised Patient: A Case ReportDaniel Alfredo Galindo ChoqueBelum ada peringkat
- Classification of Drug-Resistant Tuberculosis in An Epidemic AreaDokumen4 halamanClassification of Drug-Resistant Tuberculosis in An Epidemic AreaTika Dwi TamaBelum ada peringkat
- Perbandingan Respon Imunologi Empat Kombinasi Antiretroviral Berdasarkan Kenaikan Jumlah Cd4Dokumen7 halamanPerbandingan Respon Imunologi Empat Kombinasi Antiretroviral Berdasarkan Kenaikan Jumlah Cd4Shisii LaLaBelum ada peringkat
- Chou 2013Dokumen19 halamanChou 2013rajeshskBelum ada peringkat
- Artículo VirologíaDokumen10 halamanArtículo Virologíabrizza rodriguezBelum ada peringkat
- Cegielski, Levo Vs Moxi 3Dokumen13 halamanCegielski, Levo Vs Moxi 3hasan andrianBelum ada peringkat
- Cytomegalovirus:: Clinical Virological Correlations in Renal Transplant RecipientsDokumen10 halamanCytomegalovirus:: Clinical Virological Correlations in Renal Transplant RecipientsRaffaharianggaraBelum ada peringkat
- T L . HIV: BackgroundDokumen18 halamanT L . HIV: BackgroundOscarBelum ada peringkat
- PADDLEDokumen7 halamanPADDLEnacxit6Belum ada peringkat
- Multidrug-Resistant Tuberculosis and Culture Conversion With BedaquilineDokumen10 halamanMultidrug-Resistant Tuberculosis and Culture Conversion With BedaquilineSteven RichardBelum ada peringkat
- Nocardia Infection in KidneyDokumen20 halamanNocardia Infection in KidneysserggiosBelum ada peringkat
- Saux Et Al 2008 Quantification NRTI in Human Plasma by HPLC-MSDokumen10 halamanSaux Et Al 2008 Quantification NRTI in Human Plasma by HPLC-MSEllen Benedikta TelaumbanuaBelum ada peringkat
- Emerging Therapies in Hepatitis C. Dawn of The Era of The Direct Acting Antivirals (2011)Dokumen14 halamanEmerging Therapies in Hepatitis C. Dawn of The Era of The Direct Acting Antivirals (2011)drheayBelum ada peringkat
- Predictors of Poor Seroconversion and Adverse Events To Sars-Cov-2 Vaccine in Patients Undergoing TherapyDokumen9 halamanPredictors of Poor Seroconversion and Adverse Events To Sars-Cov-2 Vaccine in Patients Undergoing TherapySimona VisanBelum ada peringkat
- 4138 Full PDFDokumen4 halaman4138 Full PDFkarl_poorBelum ada peringkat
- Multidrug Resistant Tuberculosis Outbreak in South 7Dokumen2 halamanMultidrug Resistant Tuberculosis Outbreak in South 7Simbakutty VenkataramananBelum ada peringkat
- Lopinavir plus nucleoside reverse-transcriptase inhibitors, lopinavir plus raltegravir, or lopinavir monotherapy for second-line treatment of HIV (EARNEST) 144-week follow-up results from a randomised controlled trial - PMCDokumen24 halamanLopinavir plus nucleoside reverse-transcriptase inhibitors, lopinavir plus raltegravir, or lopinavir monotherapy for second-line treatment of HIV (EARNEST) 144-week follow-up results from a randomised controlled trial - PMCOscarBelum ada peringkat
- Jurnal 4Dokumen7 halamanJurnal 4Lutfi MalefoBelum ada peringkat
- Application of Real-Time PCR For Determination of Antiviral Drug Susceptibility of Herpes Simplex VirusDokumen5 halamanApplication of Real-Time PCR For Determination of Antiviral Drug Susceptibility of Herpes Simplex VirusMinh TriếtBelum ada peringkat
- Nejmoa 1310422Dokumen11 halamanNejmoa 1310422mz zumrodinBelum ada peringkat
- Sofosbuvir For Previously Untreated Chronic Hepatitis C InfectionDokumen23 halamanSofosbuvir For Previously Untreated Chronic Hepatitis C InfectionalfianfirdausBelum ada peringkat
- Articulo Klebsiella Pneumoniae PDFDokumen5 halamanArticulo Klebsiella Pneumoniae PDFOscarEduardoBelum ada peringkat
- Jurnal Intensified Antituberculosis Therapy in Adult With Tuberculous MeningitisDokumen13 halamanJurnal Intensified Antituberculosis Therapy in Adult With Tuberculous Meningitisnaila ghinayaBelum ada peringkat
- 1 s2.0 S0140673611609367 MainDokumen9 halaman1 s2.0 S0140673611609367 MainPraphatsorn ChaphakdeeBelum ada peringkat
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDokumen4 halamanNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiBelum ada peringkat
- Ref For Slide (4) Nosocomial InfectionsDokumen7 halamanRef For Slide (4) Nosocomial InfectionsAyesha SamnaniBelum ada peringkat
- 10 1056@NEJMoa1715849 PDFDokumen11 halaman10 1056@NEJMoa1715849 PDFdantevermillionBelum ada peringkat
- Toxicology Reports: SciencedirectDokumen6 halamanToxicology Reports: SciencedirectNoNWOBelum ada peringkat
- J. Kalita., Et Al. 2014Dokumen6 halamanJ. Kalita., Et Al. 2014Ubaida AssalwaBelum ada peringkat
- Pharmacology of HIV RXDokumen10 halamanPharmacology of HIV RXdupuytrenBelum ada peringkat
- Clinical Pharmacodynamics, Pharmacokinetics, and Drug Interaction Profile of DoravirineDokumen13 halamanClinical Pharmacodynamics, Pharmacokinetics, and Drug Interaction Profile of DoravirineFitra AlfaniBelum ada peringkat
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumDari EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumBelum ada peringkat
- ILCOR Part9 StrokeDokumen5 halamanILCOR Part9 Strokedanayanto sumbungBelum ada peringkat
- WHO Complete Hiv Report2009Dokumen150 halamanWHO Complete Hiv Report2009danayanto sumbungBelum ada peringkat
- ABC of Intensive CareDokumen49 halamanABC of Intensive CareCurro MirallesBelum ada peringkat
- Bab 198 Penggunaan Anti KoagulanDokumen4 halamanBab 198 Penggunaan Anti KoagulanRaja Alfian IrawanBelum ada peringkat
- Art 1Dokumen11 halamanArt 1danayanto sumbungBelum ada peringkat
- NVP Toxicity in Pregnant WomenDokumen5 halamanNVP Toxicity in Pregnant Womendanayanto sumbungBelum ada peringkat
- Update On ART-2010Dokumen30 halamanUpdate On ART-2010danayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
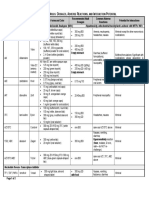
- Antiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction PotentialDokumen2 halamanAntiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction Potentialdanayanto sumbungBelum ada peringkat
- 07 Antiretroviral Drug InteractionsDokumen14 halaman07 Antiretroviral Drug Interactionsdanayanto sumbungBelum ada peringkat
- AIDS Clinical CareDokumen8 halamanAIDS Clinical Caredanayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
- CAT FFM Course Notes PDFDokumen251 halamanCAT FFM Course Notes PDFMISS AYIEEN100% (1)
- MarchDokumen1 halamanMarchSagar SiaBelum ada peringkat
- Medical TerminologyDokumen6 halamanMedical TerminologyMarhina Asarabi MukimBelum ada peringkat
- Bài tập Mệnh đề chỉ sự nhượng bộDokumen7 halamanBài tập Mệnh đề chỉ sự nhượng bộThao NguyenBelum ada peringkat
- Ken Dyne - BairnDokumen272 halamanKen Dyne - Bairnsebastien dimirdjian100% (5)
- Requirements For Correction of Clerical Error in The Middle Name or MotherDokumen1 halamanRequirements For Correction of Clerical Error in The Middle Name or MotherCecil MaquirangBelum ada peringkat
- Will Jackson CV 2018 WebsiteDokumen1 halamanWill Jackson CV 2018 Websiteapi-25454723Belum ada peringkat
- Romance Short S-WPS OfficeDokumen4 halamanRomance Short S-WPS OfficeNidya putriBelum ada peringkat
- SANLAKAS v. ReyesDokumen2 halamanSANLAKAS v. Reyesglecie_co12Belum ada peringkat
- Orthodox Calendar 2020Dokumen76 halamanOrthodox Calendar 2020ECCLESIA GOC100% (2)
- CPWD RatesDokumen197 halamanCPWD RatespnkjinamdarBelum ada peringkat
- Simran Dholasania, A200 006 948 (BIA Aug. 19, 2015)Dokumen6 halamanSimran Dholasania, A200 006 948 (BIA Aug. 19, 2015)Immigrant & Refugee Appellate Center, LLCBelum ada peringkat
- View Generated DocsDokumen2 halamanView Generated DocsMohd AhtishamBelum ada peringkat
- Maharaja Soaps industries profileDokumen41 halamanMaharaja Soaps industries profileVenki GajaBelum ada peringkat
- Case DigestDokumen11 halamanCase DigestMaLizaCainapBelum ada peringkat
- Answer KeyDokumen5 halamanAnswer KeyGurjot SinghBelum ada peringkat
- City Police Station - Space Requirements & Proximity MatrixDokumen5 halamanCity Police Station - Space Requirements & Proximity MatrixLeigh Anne VargasBelum ada peringkat
- Department of Education performance reviewDokumen22 halamanDepartment of Education performance reviewztir ecasBelum ada peringkat
- Mismatch Defect in ERW Steel Tubes: September 2014Dokumen5 halamanMismatch Defect in ERW Steel Tubes: September 2014Riza KhanBelum ada peringkat
- 3d Powerpoint TemplatesDokumen24 halaman3d Powerpoint TemplatesFarid AfrizalBelum ada peringkat
- M.Tech - Name of The Branch Seminar Presentation On "Study of Concrete Using Crumb Rubber With Partial Replacement of Fine Aggregate" Presented byDokumen17 halamanM.Tech - Name of The Branch Seminar Presentation On "Study of Concrete Using Crumb Rubber With Partial Replacement of Fine Aggregate" Presented byPrajay BhavsarBelum ada peringkat
- Long Quiz SemisDokumen2 halamanLong Quiz Semisjaja salesBelum ada peringkat
- Possible AnswersDokumen20 halamanPossible Answerssheena6Belum ada peringkat
- Greaves Cotton Non-Automotive Engines for Agriculture, Construction, Marine and Industrial ApplicationsDokumen6 halamanGreaves Cotton Non-Automotive Engines for Agriculture, Construction, Marine and Industrial ApplicationsRicardo TurlaBelum ada peringkat
- Andrew Cave, 2005. Daily Telegraph, 16 June Lifestyle SectionDokumen4 halamanAndrew Cave, 2005. Daily Telegraph, 16 June Lifestyle SectionHadi IdaBelum ada peringkat
- Divine Right - The Bilge Rat and The Mercenary Fleets of MinariaDokumen3 halamanDivine Right - The Bilge Rat and The Mercenary Fleets of MinariaScribdSucks100% (1)
- Creative Minds and CraftsDokumen162 halamanCreative Minds and CraftsLogan Mckee100% (7)
- Rod JointsDokumen27 halamanRod JointsShreyash RajBelum ada peringkat
- Student Welcome PackDokumen24 halamanStudent Welcome PackKaden MaysBelum ada peringkat
- Lesson Plan 8Dokumen3 halamanLesson Plan 8api-340707180Belum ada peringkat