Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- ILCOR Part9 StrokeDokumen5 halamanILCOR Part9 Strokedanayanto sumbungBelum ada peringkat
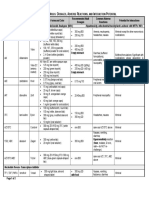
- Antiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction PotentialDokumen2 halamanAntiretroviral Drug Table - Dosages, Adverse Reactions, and Interaction Potentialdanayanto sumbungBelum ada peringkat
- ABC of Intensive CareDokumen49 halamanABC of Intensive CareCurro MirallesBelum ada peringkat
- Bab 198 Penggunaan Anti KoagulanDokumen4 halamanBab 198 Penggunaan Anti KoagulanRaja Alfian IrawanBelum ada peringkat
- 15 High Rate of Early Virological FailureDokumen9 halaman15 High Rate of Early Virological Failuredanayanto sumbungBelum ada peringkat
- Art 1Dokumen11 halamanArt 1danayanto sumbungBelum ada peringkat
- WHO Complete Hiv Report2009Dokumen150 halamanWHO Complete Hiv Report2009danayanto sumbungBelum ada peringkat
- Update On ART-2010Dokumen30 halamanUpdate On ART-2010danayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
- 07 Antiretroviral Drug InteractionsDokumen14 halaman07 Antiretroviral Drug Interactionsdanayanto sumbungBelum ada peringkat
- AIDS Clinical CareDokumen8 halamanAIDS Clinical Caredanayanto sumbungBelum ada peringkat
- 4-Mycobacterium Infection and HIVDokumen45 halaman4-Mycobacterium Infection and HIVdanayanto sumbungBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Jensen-English I SyllabusDokumen6 halamanJensen-English I Syllabusapi-284900455Belum ada peringkat
- Implementing a JITD system to reduce bullwhip effect and inventory costsDokumen7 halamanImplementing a JITD system to reduce bullwhip effect and inventory costsRaman GuptaBelum ada peringkat
- Final Exam IN Sample QuestionsDokumen27 halamanFinal Exam IN Sample QuestionsJI TEN100% (1)
- Hireena Essay AnsDokumen2 halamanHireena Essay AnsTasniiem ChandraaBelum ada peringkat
- Lewis Carrol: Birth: DeathDokumen21 halamanLewis Carrol: Birth: DeathmarialuvsjeffBelum ada peringkat
- Delhi Police ResultDokumen26 halamanDelhi Police ResultExam Aspirant100% (1)
- NVH PDFDokumen3 halamanNVH PDFSubhendu BarisalBelum ada peringkat
- DX DiagDokumen42 halamanDX DiagVinvin PatrimonioBelum ada peringkat
- Austin's Cover Letter Example - Cultivated CultureDokumen1 halamanAustin's Cover Letter Example - Cultivated CultureYash SBelum ada peringkat
- Epidemiological Cutoff Values For Antifungal Susceptibility TestingDokumen36 halamanEpidemiological Cutoff Values For Antifungal Susceptibility Testingdadrrui100% (1)
- Space 1999 Annual 1979Dokumen62 halamanSpace 1999 Annual 1979Brin Bly100% (1)
- MUM202001007 - 300 TR Price BOQ ChillerDokumen4 halamanMUM202001007 - 300 TR Price BOQ ChillerB DASBelum ada peringkat
- Hazop Recommendation Checked by FlowserveDokumen2 halamanHazop Recommendation Checked by FlowserveKareem RasmyBelum ada peringkat
- Eca Important QuestionsDokumen3 halamanEca Important QuestionsSri KrishnaBelum ada peringkat
- Causes of The Renaissance: Silk RoadDokumen6 halamanCauses of The Renaissance: Silk RoadCyryhl GutlayBelum ada peringkat
- Adjustment and Impulse Control DisordersDokumen19 halamanAdjustment and Impulse Control DisordersArchana50% (4)
- trac-nghiem-ngu-am-am-vi-hoc-tieng-anh-đã chuyển đổiDokumen18 halamantrac-nghiem-ngu-am-am-vi-hoc-tieng-anh-đã chuyển đổiNguyễn ThiênBelum ada peringkat
- Main: Exploded ViewDokumen30 halamanMain: Exploded ViewamokssantiagoBelum ada peringkat
- Srimanta Shankardev: Early LifeDokumen3 halamanSrimanta Shankardev: Early LifeAnusuya BaruahBelum ada peringkat
- Lect 1.2 Principles of Food Process DesignDokumen43 halamanLect 1.2 Principles of Food Process Designmahmoud hassanBelum ada peringkat
- Automorphic Representations and L-Functions For The General Linear Group - Volume 2cDokumen210 halamanAutomorphic Representations and L-Functions For The General Linear Group - Volume 2cluisufspaiandreBelum ada peringkat
- APA - 7thed - UCW Student Paper TemplateDokumen4 halamanAPA - 7thed - UCW Student Paper Templatesimerpreet3Belum ada peringkat
- Schedule FinalDokumen6 halamanSchedule FinalJamora ManilynBelum ada peringkat
- 2000 T.R. Higgins Award Paper - A Practical Look at Frame Analysis, Stability and Leaning ColumnsDokumen15 halaman2000 T.R. Higgins Award Paper - A Practical Look at Frame Analysis, Stability and Leaning ColumnsSamuel PintoBelum ada peringkat
- NotesTransl 108 (1985) Larsen, Who Is This GenerationDokumen20 halamanNotesTransl 108 (1985) Larsen, Who Is This GenerationluzuBelum ada peringkat
- Openstack Deployment Ops Guide PDFDokumen197 halamanOpenstack Deployment Ops Guide PDFBinank PatelBelum ada peringkat
- 05 Askeland ChapDokumen10 halaman05 Askeland ChapWeihanZhang100% (1)
- 2018 Cambridge Lower Second Progression Test Science Stage 8 QP Paper 2 - tcm143-430409Dokumen16 halaman2018 Cambridge Lower Second Progression Test Science Stage 8 QP Paper 2 - tcm143-430409AnisahBelum ada peringkat
- Datasheet AD549Dokumen14 halamanDatasheet AD549Trần Hồng VănBelum ada peringkat
- Ultra Slimpak G448-0002: Bridge Input Field Configurable IsolatorDokumen4 halamanUltra Slimpak G448-0002: Bridge Input Field Configurable IsolatorVladimirBelum ada peringkat