Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- English Proficiency TestDokumen12 halamanEnglish Proficiency Testkenjie2673% (15)
- English Proficiency TestDokumen12 halamanEnglish Proficiency Testkenjie2673% (15)
- English Proficiency TestDokumen12 halamanEnglish Proficiency Testkenjie2673% (15)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Incomplete AbortionDokumen22 halamanIncomplete AbortionAJ Dalawampu100% (2)
- Incomplete AbortionDokumen22 halamanIncomplete AbortionAJ Dalawampu100% (2)
- Organ Bath ReportDokumen13 halamanOrgan Bath ReportYusri Yusoff100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- These Colors Indicate Strength of The Solution in Parts Per Million (PPM) Available Chlorine Time of Test-1 SecondDokumen1 halamanThese Colors Indicate Strength of The Solution in Parts Per Million (PPM) Available Chlorine Time of Test-1 SecondAJ DalawampuBelum ada peringkat
- People Ware PDFDokumen8 halamanPeople Ware PDFAJ DalawampuBelum ada peringkat
- Apricot OTG User Manual8-3Dokumen36 halamanApricot OTG User Manual8-3AJ DalawampuBelum ada peringkat
- People Ware PDFDokumen8 halamanPeople Ware PDFAJ DalawampuBelum ada peringkat
- Australia Medication Safety Update 11 February 2014Dokumen8 halamanAustralia Medication Safety Update 11 February 2014AJ DalawampuBelum ada peringkat
- MS Medical WardDokumen14 halamanMS Medical WardAJ DalawampuBelum ada peringkat
- Analyzing Financial Performance ReportsDokumen5 halamanAnalyzing Financial Performance ReportsAJ DalawampuBelum ada peringkat
- Senators and Supreme Court Justices of The PhilippinesDokumen13 halamanSenators and Supreme Court Justices of The PhilippinesAJ DalawampuBelum ada peringkat
- Senators and Supreme Court Justices of The PhilippinesDokumen13 halamanSenators and Supreme Court Justices of The PhilippinesAJ DalawampuBelum ada peringkat
- Ielts App FormDokumen8 halamanIelts App FormrafavandervaartBelum ada peringkat
- Budget PrepDokumen5 halamanBudget PrepAJ DalawampuBelum ada peringkat
- Innovative School - Ezer Foundation SchoolDokumen34 halamanInnovative School - Ezer Foundation SchoolAJ DalawampuBelum ada peringkat
- NutritiDokumen12 halamanNutritiAJ DalawampuBelum ada peringkat
- Medical Surgical Nursing IDokumen11 halamanMedical Surgical Nursing IAJ DalawampuBelum ada peringkat
- Psychiatric NursingDokumen32 halamanPsychiatric NursingAJ Dalawampu100% (11)
- Lifestyle Related Diseases (LRDS) Survey FormDokumen2 halamanLifestyle Related Diseases (LRDS) Survey FormAJ DalawampuBelum ada peringkat
- 20511902Dokumen1 halaman20511902AJ DalawampuBelum ada peringkat
- Prepare For IELTSDokumen169 halamanPrepare For IELTSapi-3818413100% (2)
- Laws On Nursing PracticeDokumen2 halamanLaws On Nursing PracticeAJ DalawampuBelum ada peringkat
- Anesthetic DrugsDokumen7 halamanAnesthetic DrugsAJ DalawampuBelum ada peringkat
- Anesthetic DrugsDokumen7 halamanAnesthetic DrugsAJ DalawampuBelum ada peringkat
- DermatofibromaDokumen26 halamanDermatofibromaAJ DalawampuBelum ada peringkat
- List of Colleges and Courses ReportDokumen78 halamanList of Colleges and Courses Reportnptel nptelBelum ada peringkat
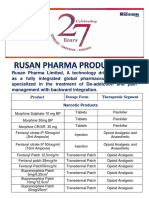
- Rusan Pharma Product ListDokumen4 halamanRusan Pharma Product ListSanjay SharmaBelum ada peringkat
- Nearest Pharmacy Delivery ServiceDokumen14 halamanNearest Pharmacy Delivery ServiceSampath WeragodaBelum ada peringkat
- Curriculo CRA PDFDokumen1 halamanCurriculo CRA PDFWamberto AlmeidaBelum ada peringkat
- Effects of Food On Drug PharmacokineticsDokumen44 halamanEffects of Food On Drug Pharmacokineticsshiploo mdBelum ada peringkat
- Dexmethylphenidate (Focalin)Dokumen2 halamanDexmethylphenidate (Focalin)Kwaku OhemengBelum ada peringkat
- Chapter-1-Introduction-Medicinal ChemistryDokumen26 halamanChapter-1-Introduction-Medicinal ChemistryFrtfBelum ada peringkat
- Farmacognosia Molecular, Lu-Qi Huang PDFDokumen233 halamanFarmacognosia Molecular, Lu-Qi Huang PDFdavidBelum ada peringkat
- Basic Marketing PlanDokumen16 halamanBasic Marketing PlanmarabillaBelum ada peringkat
- General Management of A Case of PoisoningDokumen59 halamanGeneral Management of A Case of PoisoningSudheera Rachamalla100% (1)
- GENERAL ANAESTHESIA - Presentation Editted RecordedDokumen31 halamanGENERAL ANAESTHESIA - Presentation Editted RecordedTatenda SibandaBelum ada peringkat
- Mixing InsulinDokumen2 halamanMixing Insulinadrian lozanoBelum ada peringkat
- Nexium FDADokumen22 halamanNexium FDArizkamarBelum ada peringkat
- AmantadineDokumen1 halamanAmantadinemahmoud mohamedBelum ada peringkat
- Nursing Care of The Patient With An Enteral Feeding Tube-EnFit 12-18-14Dokumen3 halamanNursing Care of The Patient With An Enteral Feeding Tube-EnFit 12-18-14barbara100% (1)
- Ketamine 1Dokumen20 halamanKetamine 1fadil23Belum ada peringkat
- Musa Paradisiaca L. and Musa Sapientum L.: A Phytochemical and Pharmacological ReviewDokumen8 halamanMusa Paradisiaca L. and Musa Sapientum L.: A Phytochemical and Pharmacological ReviewDeviBelum ada peringkat
- Antineoplastic Agents ReportDokumen3 halamanAntineoplastic Agents ReportMegan Rose MontillaBelum ada peringkat
- Pharmacology: By. Dr. Haji Bahadar, Pharmd, PHD (Pharmacology) Assistant Professor, Ipms-KmuDokumen10 halamanPharmacology: By. Dr. Haji Bahadar, Pharmd, PHD (Pharmacology) Assistant Professor, Ipms-Kmums khanBelum ada peringkat
- Fornas RS MataDokumen12 halamanFornas RS MataHery SatriawanBelum ada peringkat
- Regulatory Affairs - Pharmaceutical GuidelinesDokumen2 halamanRegulatory Affairs - Pharmaceutical Guidelinessandro CardosoBelum ada peringkat
- QuinolonesDokumen24 halamanQuinolonesKevin ArechigaBelum ada peringkat
- J Xphs 2015 12 001Dokumen9 halamanJ Xphs 2015 12 001Suprio KamalBelum ada peringkat
- Full Download Test Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition Colbert PDF Full ChapterDokumen36 halamanFull Download Test Bank For Integrated Cardiopulmonary Pharmacology 3rd Edition Colbert PDF Full Chapterpannageimban.81c15100% (18)
- Asif Mahmood's CV For Post of Lecturer PharmacyDokumen6 halamanAsif Mahmood's CV For Post of Lecturer PharmacyDr-Asif MahmoodBelum ada peringkat
- Formularium ApotekDokumen12 halamanFormularium ApotekNurul Evi kurniatiBelum ada peringkat
- Pharmaceutical Health Care IndustryDokumen120 halamanPharmaceutical Health Care IndustryJanella Garcia50% (2)
- Nausea and Vomiting in Palliative Care Audit PresentationDokumen68 halamanNausea and Vomiting in Palliative Care Audit PresentationGonzalo MaldonadoBelum ada peringkat
- Daftar Harga Ogb Januari 2021Dokumen2 halamanDaftar Harga Ogb Januari 2021rsubk sumedangBelum ada peringkat