Anda mungkin juga menyukai
- Restoration of Body Focussing On NumbersDokumen95 halamanRestoration of Body Focussing On Numbersssss87va93% (27)
- The Garlic Miracle - Discover The Amazing Health, Beauty, & Detox Benefits of This Powerful Herb (Garlic - Herbal Remedies - Herbs - Natural Cures - Home Remedies)Dokumen77 halamanThe Garlic Miracle - Discover The Amazing Health, Beauty, & Detox Benefits of This Powerful Herb (Garlic - Herbal Remedies - Herbs - Natural Cures - Home Remedies)Jowee TigasBelum ada peringkat
- Carotenoids - Food Sources, Production and Health BenefitsDokumen372 halamanCarotenoids - Food Sources, Production and Health BenefitsBernardo RodriguesBelum ada peringkat
- Cardiovascular Imaging For Clinical Practice - Nicholls e WorthleyDokumen397 halamanCardiovascular Imaging For Clinical Practice - Nicholls e WorthleyStephanie ElexiasBelum ada peringkat
- L. Stephen Coles, M.D., PH.D., Director Supercentenarian Research FoundationDokumen52 halamanL. Stephen Coles, M.D., PH.D., Director Supercentenarian Research FoundationBruceKlein100% (1)
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDokumen26 halamanAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailBelum ada peringkat
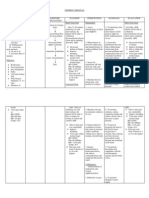
- NURSING CARE PLAN For Myocardial InfarctionDokumen13 halamanNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- Blood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlDokumen8 halamanBlood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlNovita WulandariBelum ada peringkat
- Cva CPDokumen53 halamanCva CPApol Pen100% (2)
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Dokumen70 halamanMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoBelum ada peringkat
- Care of The Chronically Ill and The Older PersonDokumen8 halamanCare of The Chronically Ill and The Older PersonAnne Con100% (1)
- Risk For Ineffective Tissue PerfusionDokumen5 halamanRisk For Ineffective Tissue PerfusionElle Oranza100% (1)
- Cardiovascular Disease and Risk Management: American Diabetes AssociationDokumen9 halamanCardiovascular Disease and Risk Management: American Diabetes AssociationIngrid DCBelum ada peringkat
- HTA en La VejezDokumen33 halamanHTA en La VejezklmflasmdaBelum ada peringkat
- 10 Curva-JcDokumen6 halaman10 Curva-Jcchandra9000Belum ada peringkat
- Perspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidenceDokumen6 halamanPerspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidencethaihavttBelum ada peringkat
- Treatment of Hypertension in Adults With Diabetes: Position StatementDokumen3 halamanTreatment of Hypertension in Adults With Diabetes: Position StatementVera WatiBelum ada peringkat
- Treatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDateDokumen34 halamanTreatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDateNiikole AcostaBelum ada peringkat
- Ciljne Vrednosti U HTADokumen2 halamanCiljne Vrednosti U HTAspalemaxBelum ada peringkat
- Hypertension in Diabetes: Treatment Considerations: Review PaperDokumen5 halamanHypertension in Diabetes: Treatment Considerations: Review Paperdivina_grace08Belum ada peringkat
- Shaikh, HT With DMDokumen9 halamanShaikh, HT With DMhasan andrianBelum ada peringkat
- s80 FullDokumen3 halamans80 FullDiego OrtechoBelum ada peringkat
- 2017 Guideline For The Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults - Key Point To RememberDokumen6 halaman2017 Guideline For The Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults - Key Point To RememberSandy Kartika PurnomoBelum ada peringkat
- DiabetesClinicalPaper en 2011Dokumen24 halamanDiabetesClinicalPaper en 2011Okky Winang SaktyawanBelum ada peringkat
- DerosaDokumen13 halamanDerosaAmeliana KamaludinBelum ada peringkat
- Aha y DiabetesDokumen9 halamanAha y DiabetesFelipe Martinez ParionaBelum ada peringkat
- 2017 Guideline For High Blood Pressure in Adults - American College of Cardiology-Key PointsDokumen7 halaman2017 Guideline For High Blood Pressure in Adults - American College of Cardiology-Key PointsRahaf K. IbrahimBelum ada peringkat
- Accord Trial Update - FinalDokumen3 halamanAccord Trial Update - FinalTyler HoffmanBelum ada peringkat
- Pencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDokumen7 halamanPencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaFarmasi RSUDBelum ada peringkat
- Eso Beta BlokerDokumen15 halamanEso Beta BlokerCarolina NauBelum ada peringkat
- UKPDS36Dokumen8 halamanUKPDS36Siskawati SuparminBelum ada peringkat
- Case Study ExamDokumen4 halamanCase Study ExamAhmed Ismail Eatmann100% (1)
- New Frontiers Hipertensi Part2Dokumen8 halamanNew Frontiers Hipertensi Part2Eunike_oisBelum ada peringkat
- Hypertensionaha 116 07090 FullDokumen2 halamanHypertensionaha 116 07090 FullYanna RizkiaBelum ada peringkat
- Blood Pressure TTR Predicts Cardiovascular Outcomes in DiabetesDokumen3 halamanBlood Pressure TTR Predicts Cardiovascular Outcomes in DiabetesGiorgi PopiashviliBelum ada peringkat
- Treatment of HypertensionDokumen23 halamanTreatment of HypertensionRABIATUL ADAWIYAHBelum ada peringkat
- Overview of Hypertension in AdultsDokumen27 halamanOverview of Hypertension in AdultsMedByteBelum ada peringkat
- AntihypertensivTreatmentElderlyVery ElderlyDokumen4 halamanAntihypertensivTreatmentElderlyVery ElderlyAn DaBelum ada peringkat
- Accepted Manuscript: The American Journal of MedicineDokumen31 halamanAccepted Manuscript: The American Journal of Medicineadel perez canenciaBelum ada peringkat
- Angiotensin-Receptor Blockers and Diuretics-Advantages of CombinationDokumen8 halamanAngiotensin-Receptor Blockers and Diuretics-Advantages of CombinationArbi SulaimanBelum ada peringkat
- Pencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDokumen7 halamanPencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDhe CoolBelum ada peringkat
- Controversies in Hypertension II: The Optimal Target Blood PressureDokumen13 halamanControversies in Hypertension II: The Optimal Target Blood PressureFideoPereBelum ada peringkat
- Hypertension 1Dokumen5 halamanHypertension 1lalitrajindoliaBelum ada peringkat
- Case HistoryDokumen8 halamanCase HistoryjabeensarwarBelum ada peringkat
- 2017-Hypertension Guidelines-AHADokumen11 halaman2017-Hypertension Guidelines-AHAIoannis KoutsodimitropoulosBelum ada peringkat
- The LancetDokumen11 halamanThe LancetBarbara Sakura RiawanBelum ada peringkat
- Fixed Combinations in The Management OLM+AmloDokumen12 halamanFixed Combinations in The Management OLM+AmloSherif AwadBelum ada peringkat
- Dci 210017Dokumen3 halamanDci 210017Gloria WuBelum ada peringkat
- Standards of Medical Care in Diabetesd2020: 10. Cardiovascular Disease and Risk ManagementDokumen24 halamanStandards of Medical Care in Diabetesd2020: 10. Cardiovascular Disease and Risk Managementcath lauuuBelum ada peringkat
- Pencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDokumen7 halamanPencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaGladys SariowanBelum ada peringkat
- 2 DR - Husna Siddiqua Thesis FinalDokumen73 halaman2 DR - Husna Siddiqua Thesis Finalcity9848835243 cyberBelum ada peringkat
- Article Abstrak Ilmiah Scientific Meeting INASH 201234Dokumen61 halamanArticle Abstrak Ilmiah Scientific Meeting INASH 201234jochebet ireneBelum ada peringkat
- Nursing Care For Patient With HypertensionDokumen13 halamanNursing Care For Patient With HypertensionSachin MadhukarBelum ada peringkat
- Diagnosis of HTN in EldersDokumen5 halamanDiagnosis of HTN in Eldersdies setyoningsihBelum ada peringkat
- Module 1 - Sample PaperDokumen7 halamanModule 1 - Sample PaperknuckleheadBelum ada peringkat
- Theassessmentandimportance Ofhypertensioninthedental SettingDokumen15 halamanTheassessmentandimportance Ofhypertensioninthedental SettingAngélica Valenzuela AndrighiBelum ada peringkat
- HTA CanadaDokumen3 halamanHTA Canadavasarhely imolaBelum ada peringkat
- تقرير ضغط الدمDokumen10 halamanتقرير ضغط الدمlyh355754Belum ada peringkat
- Diabetes, Glycemic Control, and New-Onset Heart Failure in Patients With Stable Coronary Artery DiseaseDokumen10 halamanDiabetes, Glycemic Control, and New-Onset Heart Failure in Patients With Stable Coronary Artery DiseaseEmy VishudBelum ada peringkat
- Benefits and Risks of Antihypertensive Medications in The ElderlyDokumen28 halamanBenefits and Risks of Antihypertensive Medications in The ElderlyNasrull BinHzBelum ada peringkat
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainDokumen5 halamanThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyBelum ada peringkat
- Blood Pressure and Dementia PDFDokumen15 halamanBlood Pressure and Dementia PDFeddyfadzlyBelum ada peringkat
- A Study About The Relevance of Adding Acetylsalicylic Acid in Primary Prevention in Subjects With Type 2 Diabetes MellitusDokumen13 halamanA Study About The Relevance of Adding Acetylsalicylic Acid in Primary Prevention in Subjects With Type 2 Diabetes MellitusAlfina RahmiBelum ada peringkat
- Articulo PDFDokumen8 halamanArticulo PDFKati RondonBelum ada peringkat
- Terjemahan JurnalDokumen13 halamanTerjemahan JurnalIqhe Harsono SyastrowinotoBelum ada peringkat
- HTA - Manejo - 2021Dokumen20 halamanHTA - Manejo - 2021carolina pulidoBelum ada peringkat
- Major Outcomes in High-Risk Hypertensive Patients Randomized To Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker Vs DiureticDokumen0 halamanMajor Outcomes in High-Risk Hypertensive Patients Randomized To Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker Vs DiureticFathnur SaniBelum ada peringkat
- Blood Pressure Management in Patients With DiabetesDokumen8 halamanBlood Pressure Management in Patients With DiabetesHoài ThươngBelum ada peringkat
- Case Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryDokumen9 halamanCase Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryJohn PauloBelum ada peringkat
- Hypertension: Medical Management and Nutritional ApproachesDokumen65 halamanHypertension: Medical Management and Nutritional ApproachesWelki VernandoBelum ada peringkat
- General Pathology CoopDokumen37 halamanGeneral Pathology CoopRaymondBelum ada peringkat
- Carotid ArteryDokumen5 halamanCarotid ArteryAsif AyazBelum ada peringkat
- Penyakit Arteri PeriferDokumen104 halamanPenyakit Arteri PeriferredhacuBelum ada peringkat
- IUA MLAVS Congress - Preliminary ProgrammeDokumen43 halamanIUA MLAVS Congress - Preliminary ProgrammeSFA_ANGEIOLOGIEBelum ada peringkat
- MedB Mag Interactive Vol6 PDFDokumen11 halamanMedB Mag Interactive Vol6 PDFMachi MannuBelum ada peringkat
- Roles and Mechanisms of Hawthorn and Its ExtractsDokumen12 halamanRoles and Mechanisms of Hawthorn and Its ExtractsHomer SimpsonBelum ada peringkat
- Q2 GPA Blood Vessels IIDokumen7 halamanQ2 GPA Blood Vessels IIAdrian CaballesBelum ada peringkat
- Summarized Notes Core 1 Health Priorities in AustraliaDokumen21 halamanSummarized Notes Core 1 Health Priorities in AustraliaHaBelum ada peringkat
- Describe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemDokumen4 halamanDescribe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemNathuAndrewsBelum ada peringkat
- The Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019Dokumen6 halamanThe Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019International Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Wira Gotera, DR, DR, SPPD, Kemd, Finasim Kosultan Senior, Divisi Metabolik Dan Endokrin FK Udayana-RSUP Sanglah DenpasarDokumen53 halamanWira Gotera, DR, DR, SPPD, Kemd, Finasim Kosultan Senior, Divisi Metabolik Dan Endokrin FK Udayana-RSUP Sanglah DenpasarRetno handayani PDBelum ada peringkat
- Association of Third Trimester Body Mass Index and Pregnancy Weight Gain in Obese Pregnant Women To Umbilical Artery Atherosclerotic Markers and Fetal OutcomesDokumen7 halamanAssociation of Third Trimester Body Mass Index and Pregnancy Weight Gain in Obese Pregnant Women To Umbilical Artery Atherosclerotic Markers and Fetal OutcomesMahida El shafiBelum ada peringkat
- Section 7: Problems of Oxygenation: PerfusionDokumen1 halamanSection 7: Problems of Oxygenation: PerfusionFina Sulistiawati LubisBelum ada peringkat
- CVA - Compilation of All BooksDokumen4 halamanCVA - Compilation of All BooksJohnpeter EsporlasBelum ada peringkat
- Jurnal Hiperfosfat 1Dokumen25 halamanJurnal Hiperfosfat 1Anggie Pradetya MaharaniBelum ada peringkat
- Lec10 CV PathologyDokumen75 halamanLec10 CV PathologymanuelBelum ada peringkat
- Crs Peripheral Artery Disease - Billi Brian GeniroDokumen21 halamanCrs Peripheral Artery Disease - Billi Brian Genirofathiya nurkhalisaBelum ada peringkat
- Healthmedicinet Com II 2014 FebDokumen320 halamanHealthmedicinet Com II 2014 FebHeal ThmedicinetBelum ada peringkat
- Attack, Also Called A TIA or "Mini-Stroke." A TIA Occurs IfDokumen12 halamanAttack, Also Called A TIA or "Mini-Stroke." A TIA Occurs IfMary Rose F. MalaluanBelum ada peringkat