Anda mungkin juga menyukai
- Pfo IntroDokumen9 halamanPfo IntroabdirashidBelum ada peringkat
- FRCS Exam ExperienceDokumen5 halamanFRCS Exam Experienceasi basseyBelum ada peringkat
- Management of The Floating Knee.Dokumen8 halamanManagement of The Floating Knee.barbara liuva chia policarpoBelum ada peringkat
- Basics of Knee Arthroscopy: For The BeginnersDokumen40 halamanBasics of Knee Arthroscopy: For The BeginnersPedro Zambrano100% (1)
- Guide To Trauma and Orthopaedics in SWTDokumen14 halamanGuide To Trauma and Orthopaedics in SWTapi-276370510Belum ada peringkat
- PreviewDokumen24 halamanPreviewSabryBelum ada peringkat
- Bones act as storage for calcium and phosphate but not glycogenDokumen37 halamanBones act as storage for calcium and phosphate but not glycogenvisfralin100% (1)
- Alingment in TKRDokumen3 halamanAlingment in TKRdeepak100% (1)
- Ortho AIIMSDokumen15 halamanOrtho AIIMSvkBelum ada peringkat
- Customers Who Viewed Also Viewed: Paperback - 10 December 2017Dokumen4 halamanCustomers Who Viewed Also Viewed: Paperback - 10 December 2017Rajesh Itha100% (1)
- OKU Referat Bedah PDFDokumen469 halamanOKU Referat Bedah PDFAde ZulfiahBelum ada peringkat
- Crozer-Keystone Ex Tern Ship ManualDokumen187 halamanCrozer-Keystone Ex Tern Ship ManualRihamary CruzBelum ada peringkat
- 2016 OITE Study Guide For ResidentsDokumen273 halaman2016 OITE Study Guide For Residentschu_chiang_3100% (1)
- DNB Orthopaedics Theory PapersDokumen23 halamanDNB Orthopaedics Theory PapersmystraviBelum ada peringkat
- Hand OITE Questions for NYSSH Update Course 2007Dokumen35 halamanHand OITE Questions for NYSSH Update Course 2007ICH KhuyBelum ada peringkat
- Orthopedic VIVA Made Easy: November 2020Dokumen15 halamanOrthopedic VIVA Made Easy: November 2020EmailBelum ada peringkat
- Fungal Nail and Ingrown Toenail GuideDokumen60 halamanFungal Nail and Ingrown Toenail GuideAmar AlkhafajiBelum ada peringkat
- OITE 2006 Questions For Nyssh UpdateDokumen31 halamanOITE 2006 Questions For Nyssh UpdateICH KhuyBelum ada peringkat
- M.S. Orthopaedic Surgery SyllabusDokumen8 halamanM.S. Orthopaedic Surgery SyllabusMuthu KumarBelum ada peringkat
- Pediatric Knee Injuries: Greg M. Osgood, MDDokumen101 halamanPediatric Knee Injuries: Greg M. Osgood, MDkosmynin86100% (1)
- @MedicalBooksStore 2013 ExternalDokumen431 halaman@MedicalBooksStore 2013 ExternalОлександр ШендераBelum ada peringkat
- Approach To FractureDokumen17 halamanApproach To FractureRebecca WongBelum ada peringkat
- Basic Science OITE ReviewDokumen91 halamanBasic Science OITE ReviewICH KhuyBelum ada peringkat
- Orthopaedics PunchDokumen6 halamanOrthopaedics PunchHicham GawishBelum ada peringkat
- Gpe - 017.1 - Orthopaedic ExaminationDokumen3 halamanGpe - 017.1 - Orthopaedic ExaminationImiey Eleena HanumBelum ada peringkat
- Modified French OsteotomyDokumen5 halamanModified French OsteotomyKaustubh KeskarBelum ada peringkat
- AAOS Anatomy 2008Dokumen63 halamanAAOS Anatomy 2008Dr-fadi AlkhasawnehBelum ada peringkat
- Orthopedics Oath C1 Mini-OSCEDokumen5 halamanOrthopedics Oath C1 Mini-OSCEHajar AlajlouniBelum ada peringkat
- Fractures and Dislocations About The Elbow in The Pediatric PatientDokumen65 halamanFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaBelum ada peringkat
- Deformities of the Great and Lesser Toes: Hammer Toe, Claw Toe, Hallux Valgus, Hallux Rigidus and Mallet ToeDokumen20 halamanDeformities of the Great and Lesser Toes: Hammer Toe, Claw Toe, Hallux Valgus, Hallux Rigidus and Mallet ToeSylvia ChongBelum ada peringkat
- Hand OITE - 2012 2013 2014Dokumen209 halamanHand OITE - 2012 2013 2014Sadiq AliBelum ada peringkat
- 5 6082210811156103668Dokumen659 halaman5 6082210811156103668Guilherme Pellisson FavarettoBelum ada peringkat
- Orthopedics: Notes, 1/eDokumen26 halamanOrthopedics: Notes, 1/evkBelum ada peringkat
- AAOS Spine 2009 PDFDokumen174 halamanAAOS Spine 2009 PDFDr-fadi AlkhasawnehBelum ada peringkat
- G11-Principles of External FixationDokumen108 halamanG11-Principles of External FixationIkram HussainBelum ada peringkat
- Osteotomies Around The Knee Indications-Planning-Surgical T111Dokumen300 halamanOsteotomies Around The Knee Indications-Planning-Surgical T111jo chenBelum ada peringkat
- AO-ASIF - Instruments & ImplantsDokumen582 halamanAO-ASIF - Instruments & ImplantsthiagoBelum ada peringkat
- Mallet Finger Suturing TechniqueDokumen5 halamanMallet Finger Suturing TechniqueSivaprasath JaganathanBelum ada peringkat
- Practical ProceduresDokumen315 halamanPractical ProceduresAnil SoodBelum ada peringkat
- Handbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFDokumen6 halamanHandbook of Foot and Ankle Orthopedics (Rational Prescription of Foot and Ankle Orthotics) PDFAbdallah Jaber100% (2)
- Lateral Condyle Fracture Tips and TricksDokumen33 halamanLateral Condyle Fracture Tips and TricksPurushotham NalamatiBelum ada peringkat
- Module 2 OrthopedicsDokumen50 halamanModule 2 Orthopedicspjanu86Belum ada peringkat
- Screw PlacementDokumen32 halamanScrew PlacementDraconian1Belum ada peringkat
- Orthoheal - DNB Ortho Theory Question Papers AnalysisDokumen29 halamanOrthoheal - DNB Ortho Theory Question Papers AnalysisSivaprasath JaganathanBelum ada peringkat
- Osteomyelitis in Long BonesDokumen14 halamanOsteomyelitis in Long BonesAstary PasorongBelum ada peringkat
- DR - O. K. A. SamuelsDokumen76 halamanDR - O. K. A. Samuelsgdudex118811Belum ada peringkat
- MPFL ReconstructionDokumen16 halamanMPFL ReconstructiondrjorgewtorresBelum ada peringkat
- AAOS2012 Foot and AnkleDokumen103 halamanAAOS2012 Foot and AnkleAmmar HilliBelum ada peringkat
- Antibiotic Classification & Mechanism - Basic Science - OrthobulletsDokumen7 halamanAntibiotic Classification & Mechanism - Basic Science - OrthobulletsYuttapol PimpisonBelum ada peringkat
- Bone Transport Distraction Osteogenesis 1Dokumen31 halamanBone Transport Distraction Osteogenesis 1Euginia YosephineBelum ada peringkat
- Common CasesDokumen44 halamanCommon CasesRebecca WongBelum ada peringkat
- Atlas of Internal Fixation - Fractures of Long Bones. Classification, Statistical Analysis, Technique, Radiology (PDFDrive)Dokumen350 halamanAtlas of Internal Fixation - Fractures of Long Bones. Classification, Statistical Analysis, Technique, Radiology (PDFDrive)SANDEEPBelum ada peringkat
- Clinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtDokumen29 halamanClinical Management of Hip Arthroplasty: Kiefer Usbeck Scheuber AtzrodtGlauber Teixeira ErvilhaBelum ada peringkat
- The Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSDokumen7 halamanThe Timed Up & Go - A Test of Basic Functional Mobility For Frail Elderly Persons. lAGSJose Fernando Díez ConchaBelum ada peringkat
- MILLER Testable ConceptsDokumen109 halamanMILLER Testable ConceptsMohammedGooda100% (1)
- PDFDokumen328 halamanPDFBreak DerulsBelum ada peringkat
- Orthopaedic Management in Cerebral Palsy, 2nd EditionDari EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannPenilaian: 3 dari 5 bintang3/5 (2)
- Bone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsDari EverandBone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsBelum ada peringkat
- MODIFIED POSTERIOR APPROACH TO THE HIP JOINTDari EverandMODIFIED POSTERIOR APPROACH TO THE HIP JOINTPenilaian: 5 dari 5 bintang5/5 (1)
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionDari EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionBelum ada peringkat
- Meta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingDokumen21 halamanMeta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingTyler Lawrence CoyeBelum ada peringkat
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Dokumen3 halamanLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeBelum ada peringkat
- Jfas Original ResearchDokumen12 halamanJfas Original ResearchTyler Lawrence CoyeBelum ada peringkat
- Podiatry Institute ManualDokumen301 halamanPodiatry Institute ManualTyler Lawrence Coye100% (2)
- Treatment of Lisfranc Fracture-Dislocations With PDokumen8 halamanTreatment of Lisfranc Fracture-Dislocations With PTyler Lawrence CoyeBelum ada peringkat
- Dfa 6 29629Dokumen12 halamanDfa 6 29629Tyler Lawrence CoyeBelum ada peringkat
- Anki Data Folder Location and Backup GuideDokumen1 halamanAnki Data Folder Location and Backup GuideTyler Lawrence CoyeBelum ada peringkat
- Ankle Instability 2017-2018Dokumen44 halamanAnkle Instability 2017-2018Tyler Lawrence CoyeBelum ada peringkat
- Anti EpilepticsDokumen46 halamanAnti EpilepticsTyler Lawrence CoyeBelum ada peringkat
- Trauma Manual (Podiatry)Dokumen403 halamanTrauma Manual (Podiatry)QuantumjanitorBelum ada peringkat
- Penn Presby Residency Manual PodiatryDokumen400 halamanPenn Presby Residency Manual PodiatryTyler Lawrence Coye100% (1)
- Wound and Skin Ulcer Management Care Guide PDFDokumen21 halamanWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngBelum ada peringkat
- Trauma Workshop 1Dokumen10 halamanTrauma Workshop 1Tyler Lawrence CoyeBelum ada peringkat
- AntipsychoticsDokumen29 halamanAntipsychoticsTyler Lawrence Coye100% (4)
- Lecture 3 Capsule Tendon Balance ProceduresDokumen19 halamanLecture 3 Capsule Tendon Balance ProceduresTyler Lawrence CoyeBelum ada peringkat
- AnticoagulantsDokumen47 halamanAnticoagulantsTyler Lawrence Coye100% (1)
- Principles of ankle and foot CT imaging and applicationsDokumen48 halamanPrinciples of ankle and foot CT imaging and applicationsTyler Lawrence CoyeBelum ada peringkat
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDokumen16 halamanThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- The Ohio Book - LEA DiagramsDokumen168 halamanThe Ohio Book - LEA DiagramsTyler Lawrence Coye100% (2)
- 09 Vascular TraumaDokumen36 halaman09 Vascular TraumaTyler Lawrence CoyeBelum ada peringkat
- Venous DiseaseDokumen19 halamanVenous DiseaseTyler Lawrence CoyeBelum ada peringkat
- Mit PDFDokumen106 halamanMit PDFTyler Lawrence CoyeBelum ada peringkat
- USMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionDokumen36 halamanUSMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionTyler Lawrence CoyeBelum ada peringkat
- Lecture-12-2 22 17Dokumen7 halamanLecture-12-2 22 17Tyler Lawrence CoyeBelum ada peringkat
- Respratory Drugs I-IIDokumen10 halamanRespratory Drugs I-IITyler Lawrence CoyeBelum ada peringkat
- CROZER-KEYSTONE RESIDENCY MANUAL SECOND EDITIONDokumen219 halamanCROZER-KEYSTONE RESIDENCY MANUAL SECOND EDITIONTyler Lawrence CoyeBelum ada peringkat
- Drugs Class Mechanism: Guaifenesin (OTC)Dokumen10 halamanDrugs Class Mechanism: Guaifenesin (OTC)Tyler Lawrence CoyeBelum ada peringkat
- Anatomy RecallDokumen337 halamanAnatomy RecallTyler Lawrence Coye100% (2)
- Chapter 8 - Head and Neck 2015Dokumen72 halamanChapter 8 - Head and Neck 2015Tyler Lawrence CoyeBelum ada peringkat
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDokumen4 halamanChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZBelum ada peringkat
- Electrocardiography Wave Analysis: Using MATLABDokumen19 halamanElectrocardiography Wave Analysis: Using MATLABSMBelum ada peringkat
- Int Obs PDFDokumen37 halamanInt Obs PDFsurgeon77Belum ada peringkat
- IV Therapy SsDokumen56 halamanIV Therapy Sssaeed_chohan100% (8)
- CDN 1 PDFDokumen22 halamanCDN 1 PDFJohn Mark100% (1)
- Definition of NephrolithiasisDokumen30 halamanDefinition of Nephrolithiasiszz_13Belum ada peringkat
- Acute Kidney Injury W/ Hyperkalemia NCPDokumen5 halamanAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenBelum ada peringkat
- Unipex Onepager CapixylDokumen1 halamanUnipex Onepager CapixylalbertitorubinBelum ada peringkat
- Type2 Diabetes HandoutDokumen1 halamanType2 Diabetes Handouthendra_darmawan_4Belum ada peringkat
- PrimaquineDokumen3 halamanPrimaquineVijayakumar NsBelum ada peringkat
- Role of Autologous Platelet-Rich Plasma in Z-PlastyDokumen3 halamanRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsBelum ada peringkat
- Effect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFDokumen3 halamanEffect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFyolandaBelum ada peringkat
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDokumen8 halamanVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengBelum ada peringkat
- English Intervention DialogueDokumen3 halamanEnglish Intervention DialogueJihan Irbah TrianiBelum ada peringkat
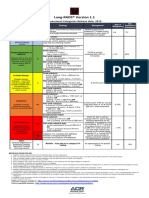
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- Case Study PneumothoraxDokumen9 halamanCase Study PneumothoraxLee_Cabral_693967% (3)
- Dementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyDokumen9 halamanDementia Incidence, Burden and Cost of Care: A Filipino Community-Based StudyVanessa PalomaBelum ada peringkat
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDokumen21 halamanChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoBelum ada peringkat
- Eric Berg CVDokumen6 halamanEric Berg CVHaralambicBelum ada peringkat
- OSCE Chart Cough (KK)Dokumen4 halamanOSCE Chart Cough (KK)api-26938624Belum ada peringkat
- 13 - Adverse Drug Reactions CausesDokumen4 halaman13 - Adverse Drug Reactions CausesRojas Evert AlonsoBelum ada peringkat
- Feline Asthma: Laura A. Nafe, DVM, MS, Dacvim (Saim)Dokumen5 halamanFeline Asthma: Laura A. Nafe, DVM, MS, Dacvim (Saim)Miruna ChiriacBelum ada peringkat
- Ligibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineDokumen20 halamanLigibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineJasmyn KimBelum ada peringkat
- Dental Perspective of Pemphigus VulgarisDokumen5 halamanDental Perspective of Pemphigus VulgarisSherlyBelum ada peringkat
- Source Control in Emergency General SurgeryDokumen21 halamanSource Control in Emergency General SurgerylaviniaBelum ada peringkat
- Transverse Dimension Diagnosis and Relevance to Functional OcclusionDokumen6 halamanTransverse Dimension Diagnosis and Relevance to Functional OcclusionDino MainoBelum ada peringkat
- Nephrons (Functional Unit)Dokumen44 halamanNephrons (Functional Unit)Nur SanaaniBelum ada peringkat
- Volume 43, Number 12, March 23, 2012Dokumen56 halamanVolume 43, Number 12, March 23, 2012BladeBelum ada peringkat
- Myocardial InfarctionDokumen18 halamanMyocardial InfarctionMarc Lorenz DucusinBelum ada peringkat
- B. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseDokumen4 halamanB. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseSOLEIL LOUISE LACSON MARBAS100% (1)