Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- An Analysis of The Cloud Computing Security ProblemDokumen6 halamanAn Analysis of The Cloud Computing Security Problemrmsaqib1Belum ada peringkat
- Statistics Without Tears by Stan BrownDokumen294 halamanStatistics Without Tears by Stan BrownlovehackinggalsBelum ada peringkat
- LhiannanDokumen6 halamanLhiannanGreybornBelum ada peringkat
- Robert Egby - DecreesDokumen9 halamanRobert Egby - DecreesmuzickaueBelum ada peringkat
- Preboard Practice PDFDokumen25 halamanPreboard Practice PDFGracielle NebresBelum ada peringkat
- Matter Around Me: SC1 - Teaching Science in ElementaryDokumen27 halamanMatter Around Me: SC1 - Teaching Science in ElementaryYanna Marie Porlucas Macaraeg50% (2)
- 4.9 Design of Compression Members: L 4.7 UsingDokumen22 halaman4.9 Design of Compression Members: L 4.7 Usingctc1212100% (1)
- Technical Data - Tad1342veDokumen9 halamanTechnical Data - Tad1342veRachid SmailiBelum ada peringkat
- Aits 2122 PT I Jeea 2022 TD Paper 2 SolDokumen14 halamanAits 2122 PT I Jeea 2022 TD Paper 2 SolSoumodeep NayakBelum ada peringkat
- English 8 q3 w1 6 FinalDokumen48 halamanEnglish 8 q3 w1 6 FinalJedidiah NavarreteBelum ada peringkat
- Millennium Development GoalsDokumen6 halamanMillennium Development GoalsSasha Perera100% (2)
- Jurnal KORELASI ANTARA STATUS GIZI IBU MENYUSUI DENGAN KECUKUPAN ASIDokumen9 halamanJurnal KORELASI ANTARA STATUS GIZI IBU MENYUSUI DENGAN KECUKUPAN ASIMarsaidBelum ada peringkat
- A Wicked Game by Kate BatemanDokumen239 halamanA Wicked Game by Kate BatemanNevena Nikolic100% (1)
- Printed The Strange Case of DR Jekyll & MR HydeDokumen96 halamanPrinted The Strange Case of DR Jekyll & MR HydelovehackinggalsBelum ada peringkat
- Diagnostic Test Everybody Up 5, 2020Dokumen2 halamanDiagnostic Test Everybody Up 5, 2020George Paz0% (1)
- 1823-From PortalDokumen4 halaman1823-From PortallovehackinggalsBelum ada peringkat
- Negotations Post TenderDokumen3 halamanNegotations Post TenderlovehackinggalsBelum ada peringkat
- SP 46 EngineeringDrawing Practice For Schools and Colleges PDFDokumen213 halamanSP 46 EngineeringDrawing Practice For Schools and Colleges PDFlovehackinggalsBelum ada peringkat
- Is 808Dokumen60 halamanIs 808lovehackinggalsBelum ada peringkat
- IS 1200 Part 9Dokumen11 halamanIS 1200 Part 9lovehackinggalsBelum ada peringkat
- Grant of Completion Certificate Under The Lease & Execution of Perpetual LeaseDokumen1 halamanGrant of Completion Certificate Under The Lease & Execution of Perpetual LeaselovehackinggalsBelum ada peringkat
- Is 12778Dokumen17 halamanIs 12778lovehackinggalsBelum ada peringkat
- Is 17372 2020Dokumen12 halamanIs 17372 2020lovehackinggals100% (1)
- Additional Construction in Open Areas in Connaught PlaceDokumen1 halamanAdditional Construction in Open Areas in Connaught PlacelovehackinggalsBelum ada peringkat
- Inspection of PropertiesDokumen2 halamanInspection of PropertieslovehackinggalsBelum ada peringkat
- Cost of Preparation of Various DocumentsDokumen3 halamanCost of Preparation of Various DocumentslovehackinggalsBelum ada peringkat
- Duties Responsibilities of Various Officers andDokumen18 halamanDuties Responsibilities of Various Officers andSita RamBelum ada peringkat
- Allotment of LandDokumen7 halamanAllotment of LandlovehackinggalsBelum ada peringkat
- Chapter-18 Breaches (Change of Purpose or Unauthorised Construction)Dokumen3 halamanChapter-18 Breaches (Change of Purpose or Unauthorised Construction)lovehackinggalsBelum ada peringkat
- Sanction of Plans Under The LeaseDokumen2 halamanSanction of Plans Under The LeaselovehackinggalsBelum ada peringkat
- Acquisition of LandDokumen1 halamanAcquisition of LandlovehackinggalsBelum ada peringkat
- Scrutinisation of Building PlanDokumen1 halamanScrutinisation of Building PlanlovehackinggalsBelum ada peringkat
- Additional ConstructionDokumen3 halamanAdditional ConstructionlovehackinggalsBelum ada peringkat
- Permanent Chnage of PurposeDokumen1 halamanPermanent Chnage of PurposelovehackinggalsBelum ada peringkat
- Sub-Division of PlotsDokumen4 halamanSub-Division of PlotslovehackinggalsBelum ada peringkat
- CEHv10 Module 01 Introduction To Ethical HackingDokumen157 halamanCEHv10 Module 01 Introduction To Ethical Hackinglovehackinggals100% (1)
- Delegation of PowersDokumen4 halamanDelegation of PowerslovehackinggalsBelum ada peringkat
- Demarcation & Handing Over Possession of LandDokumen1 halamanDemarcation & Handing Over Possession of LandlovehackinggalsBelum ada peringkat
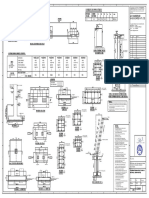
- S - 3001 Foundatiom and Details (Main Gate) - ModelDokumen1 halamanS - 3001 Foundatiom and Details (Main Gate) - ModellovehackinggalsBelum ada peringkat
- Prospectus: (A Statutory Body Under Ministry of Power, Government of India)Dokumen22 halamanProspectus: (A Statutory Body Under Ministry of Power, Government of India)skredhu56789Belum ada peringkat
- Types of LeasesDokumen2 halamanTypes of LeaseslovehackinggalsBelum ada peringkat
- The Energy Conservation Act, 2001 No 52 2001: Ministry of Law, Justice and Company AffairsDokumen22 halamanThe Energy Conservation Act, 2001 No 52 2001: Ministry of Law, Justice and Company Affairssumitsonu4uBelum ada peringkat
- Digitally Signed: RAKESH KUMAR RAI Sun Mar 01 10:55:07 IST 2020 Secretary, BEE New DelhiDokumen1 halamanDigitally Signed: RAKESH KUMAR RAI Sun Mar 01 10:55:07 IST 2020 Secretary, BEE New DelhilovehackinggalsBelum ada peringkat
- EQUIP9-Operations-Use Case ChallengeDokumen6 halamanEQUIP9-Operations-Use Case ChallengeTushar ChaudhariBelum ada peringkat
- Promoting The Conservation and Use of Under Utilized and Neglected Crops. 12 - TefDokumen52 halamanPromoting The Conservation and Use of Under Utilized and Neglected Crops. 12 - TefEduardo Antonio Molinari NovoaBelum ada peringkat
- 1 s2.0 S0378432004002465 MainDokumen20 halaman1 s2.0 S0378432004002465 MainMuhammad JameelBelum ada peringkat
- Annotated Bibliography 2Dokumen3 halamanAnnotated Bibliography 2api-458997989Belum ada peringkat
- James KlotzDokumen2 halamanJames KlotzMargaret ElwellBelum ada peringkat
- Comparison of Multi-Coil and Diaphragm Spring ClutchesDokumen3 halamanComparison of Multi-Coil and Diaphragm Spring Clutchesmasb_994077Belum ada peringkat
- 3114 Entrance-Door-Sensor 10 18 18Dokumen5 halaman3114 Entrance-Door-Sensor 10 18 18Hamilton Amilcar MirandaBelum ada peringkat
- The Story of An Hour QuestionpoolDokumen5 halamanThe Story of An Hour QuestionpoolAKM pro player 2019Belum ada peringkat
- (Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)Dokumen192 halaman(Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)BrunoRamosdeLima100% (1)
- Photoshoot Plan SheetDokumen1 halamanPhotoshoot Plan Sheetapi-265375120Belum ada peringkat
- Ingres in ReproductionDokumen20 halamanIngres in ReproductionKarlBelum ada peringkat
- -4618918اسئلة مدني فحص التخطيط مع الأجوبة من د. طارق الشامي & م. أحمد هنداويDokumen35 halaman-4618918اسئلة مدني فحص التخطيط مع الأجوبة من د. طارق الشامي & م. أحمد هنداويAboalmaail Alamin100% (1)
- Term Paper A and CDokumen9 halamanTerm Paper A and CKishaloy NathBelum ada peringkat
- SST Vs BBTDokumen7 halamanSST Vs BBTFlaxkikare100% (1)
- The Evolution of Knowledge Management Systems Needs To Be ManagedDokumen14 halamanThe Evolution of Knowledge Management Systems Needs To Be ManagedhenaediBelum ada peringkat
- Discrete Random Variables: 4.1 Definition, Mean and VarianceDokumen15 halamanDiscrete Random Variables: 4.1 Definition, Mean and VariancejordyswannBelum ada peringkat
- Award Presentation Speech PDFDokumen3 halamanAward Presentation Speech PDFNehal RaiBelum ada peringkat