Anda mungkin juga menyukai
- Adictos A Internet en RehabilitacionDokumen7 halamanAdictos A Internet en RehabilitacionDante LunaBelum ada peringkat
- Revista Latinoamericana de PsicologíaDokumen14 halamanRevista Latinoamericana de PsicologíaDante LunaBelum ada peringkat
- Anhedonia Vs IGA AdultosDokumen3 halamanAnhedonia Vs IGA AdultosDante LunaBelum ada peringkat
- Adiccion y Depression en AdolescentesDokumen8 halamanAdiccion y Depression en AdolescentesDante LunaBelum ada peringkat
- Adictos A Internet en RehabilitacionDokumen7 halamanAdictos A Internet en RehabilitacionDante LunaBelum ada peringkat
- IGA TratamientoDokumen8 halamanIGA TratamientoDante LunaBelum ada peringkat
- International Journal of Clinical and Health PsychologyDokumen6 halamanInternational Journal of Clinical and Health PsychologyDante LunaBelum ada peringkat
- 3Dokumen10 halaman3Dante LunaBelum ada peringkat
- Adiccion Vs Depression Adultos y AdolescentesDokumen6 halamanAdiccion Vs Depression Adultos y AdolescentesDante LunaBelum ada peringkat
- Adictos A Internet en RehabilitacionDokumen7 halamanAdictos A Internet en RehabilitacionDante LunaBelum ada peringkat
- Articulo 2Dokumen12 halamanArticulo 2Dante LunaBelum ada peringkat
- Clínica y Salud: Functional Analytic Psychotherapy Among Mothers With Children With Disruptive BehaviorDokumen7 halamanClínica y Salud: Functional Analytic Psychotherapy Among Mothers With Children With Disruptive BehaviorDante LunaBelum ada peringkat
- Estudiantes Nigerianos Internet Addiction Vs DepressionDokumen9 halamanEstudiantes Nigerianos Internet Addiction Vs DepressionDante LunaBelum ada peringkat
- Adicction Vs Depression World SurveyDokumen64 halamanAdicction Vs Depression World SurveyDante LunaBelum ada peringkat
- Adiccion y Personalidad DepresivaDokumen9 halamanAdiccion y Personalidad DepresivaDante LunaBelum ada peringkat
- Comorbidity IGA Vs Anxiety and DepressionDokumen3 halamanComorbidity IGA Vs Anxiety and DepressionDante LunaBelum ada peringkat
- IGA TratamientoDokumen8 halamanIGA TratamientoDante LunaBelum ada peringkat
- Anhedonia Vs IGA AdultosDokumen3 halamanAnhedonia Vs IGA AdultosDante LunaBelum ada peringkat
- Adiccion y Depression en AdolescentesDokumen8 halamanAdiccion y Depression en AdolescentesDante LunaBelum ada peringkat
- Adiccion Vs Depression Adultos y AdolescentesDokumen6 halamanAdiccion Vs Depression Adultos y AdolescentesDante LunaBelum ada peringkat
- Correlation Depression Vs Internet UseDokumen7 halamanCorrelation Depression Vs Internet UseDante LunaBelum ada peringkat
- Grados de Adiccion y Depresion en ChinosDokumen7 halamanGrados de Adiccion y Depresion en ChinosDante LunaBelum ada peringkat
- Internet AddictionDokumen5 halamanInternet AddictionNurul NurulatikahBelum ada peringkat
- Clinical Psychology Review: Daniel L. King, Paul H. DelfabbroDokumen11 halamanClinical Psychology Review: Daniel L. King, Paul H. DelfabbroLinyak 2509Belum ada peringkat
- IGA Analisis PsiquiatricoDokumen25 halamanIGA Analisis PsiquiatricoDante LunaBelum ada peringkat
- IGA Ninos MumbaiDokumen4 halamanIGA Ninos MumbaiDante LunaBelum ada peringkat
- Pathological Video Game Use Among Youths: A Two-Year Longitudinal StudyDokumen13 halamanPathological Video Game Use Among Youths: A Two-Year Longitudinal StudyDante LunaBelum ada peringkat
- IGA Estudiantes de Medicina Vs Depression PDFDokumen10 halamanIGA Estudiantes de Medicina Vs Depression PDFDante LunaBelum ada peringkat
- Pathological Video Game Use Among Youths: A Two-Year Longitudinal StudyDokumen13 halamanPathological Video Game Use Among Youths: A Two-Year Longitudinal StudyDante LunaBelum ada peringkat
- IGA Vs Sintomatologia DepresivaDokumen14 halamanIGA Vs Sintomatologia DepresivaDante LunaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Административная контрольная работа по английскому (7 класс)Dokumen2 halamanАдминистративная контрольная работа по английскому (7 класс)AlexKubrickBelum ada peringkat
- Cbydp & AbyipDokumen17 halamanCbydp & AbyipJanine PigaoBelum ada peringkat
- HN Webinar Healthy Gut Healthy You November 2023Dokumen39 halamanHN Webinar Healthy Gut Healthy You November 2023ramcm024Belum ada peringkat
- CAUSES OF EXCESS FLOOD IN UYO LOCAL GOVERNMENT AREA - UniProjectMaterialsDokumen3 halamanCAUSES OF EXCESS FLOOD IN UYO LOCAL GOVERNMENT AREA - UniProjectMaterialsabdulBelum ada peringkat
- FORMULATION DEVELOPMENT OF FLOATING DRUG DELIVERY SYSTEM (FDDS) FOR LAFUTIDINE C.V.S.Raghu Kiran, C.GopinathDokumen7 halamanFORMULATION DEVELOPMENT OF FLOATING DRUG DELIVERY SYSTEM (FDDS) FOR LAFUTIDINE C.V.S.Raghu Kiran, C.GopinathiajpsBelum ada peringkat
- Government Chengalpattu Medical College and Hospital: GCMCK 303504929 3373001366102Dokumen1 halamanGovernment Chengalpattu Medical College and Hospital: GCMCK 303504929 3373001366102Ms DhoniBelum ada peringkat
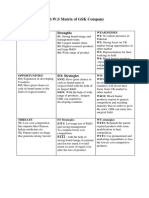
- Tows GSKDokumen2 halamanTows GSKQanita Shah100% (2)
- Aust Dental Council Strategic Plan - '16-'19Dokumen2 halamanAust Dental Council Strategic Plan - '16-'19Anup Lal RajbahakBelum ada peringkat
- Chlorine, Free: Usepa DPD Method Method 10245 0.05 To 4.00 MG/L CL (MR) Powder PillowsDokumen6 halamanChlorine, Free: Usepa DPD Method Method 10245 0.05 To 4.00 MG/L CL (MR) Powder PillowsPedro MamaniBelum ada peringkat
- Guidelines On The Training of Ship's cooks-ILO PDFDokumen66 halamanGuidelines On The Training of Ship's cooks-ILO PDFBisratBelum ada peringkat
- Finalresume Edrielle 2 CsitDokumen1 halamanFinalresume Edrielle 2 Csitapi-343765009Belum ada peringkat
- 75 Items To Stockpile Before The CollapseDokumen40 halaman75 Items To Stockpile Before The CollapseMely100% (3)
- COVID-19 Pandemic, Socioeconomic Crisis and Human Stress inDokumen12 halamanCOVID-19 Pandemic, Socioeconomic Crisis and Human Stress inMaisha Tabassum AnimaBelum ada peringkat
- Make Mental Wellbeing Top PriorityDokumen1 halamanMake Mental Wellbeing Top PrioritySamatha RobertsBelum ada peringkat
- Renal Transplant ProtocolsDokumen42 halamanRenal Transplant ProtocolsParis VlachosBelum ada peringkat
- Issue 26 - The Nurse Advocate - Hamad Medical Corporation - July 2016Dokumen20 halamanIssue 26 - The Nurse Advocate - Hamad Medical Corporation - July 2016Brent ForemanBelum ada peringkat
- Evaluate Hazards and RisksDokumen17 halamanEvaluate Hazards and RisksJENEFER REYESBelum ada peringkat
- Albert Bandura 4 Sources of Influence To Develop Self EfficacyDokumen2 halamanAlbert Bandura 4 Sources of Influence To Develop Self EfficacySabio Evan JesusBelum ada peringkat
- Neonatal Incubator en B8B6 V1.2Dokumen8 halamanNeonatal Incubator en B8B6 V1.2Surta DevianaBelum ada peringkat
- 807 Model Answer Winter 2017Dokumen24 halaman807 Model Answer Winter 2017Mahesh DeshmukhBelum ada peringkat
- The Case of George EthicsDokumen4 halamanThe Case of George EthicsPau De GuzmanBelum ada peringkat
- GURPS 4e - (Unofficial) Warhammer PDFDokumen8 halamanGURPS 4e - (Unofficial) Warhammer PDFBruno CelhoBelum ada peringkat
- Peak Fitness WorkoutDokumen6 halamanPeak Fitness WorkoutIsael AlemanBelum ada peringkat
- Harga Obat MahakamDokumen4 halamanHarga Obat Mahakammuhammad ubaidillahBelum ada peringkat
- Barangay Disaster Risk Reduction Management PlanDokumen25 halamanBarangay Disaster Risk Reduction Management PlanGain Gain100% (1)
- Near Miss Training ProgramDokumen45 halamanNear Miss Training ProgramSabeehul RehmanBelum ada peringkat
- Social Networking Enjoyment's Dual EffectsDokumen17 halamanSocial Networking Enjoyment's Dual EffectsMaverick Hunter RezaBelum ada peringkat
- Micronutrient Deficiencies ExplainedDokumen34 halamanMicronutrient Deficiencies ExplainedRegita Trimulia100% (1)
- SJ IH1 MinutesDokumen5 halamanSJ IH1 MinutesKirsten NVBelum ada peringkat
- ResumeDokumen2 halamanResumeapi-601587526Belum ada peringkat