Anda mungkin juga menyukai
- Brain Sciences: Thiamine Deficiency Causes Long-Lasting Neurobehavioral Deficits in MiceDokumen15 halamanBrain Sciences: Thiamine Deficiency Causes Long-Lasting Neurobehavioral Deficits in MiceAnonymous ORleRrBelum ada peringkat
- X 9702500504Dokumen6 halamanX 9702500504Anonymous ORleRrBelum ada peringkat
- Is Venous Congestion Associated With Reduced Cerebral Oxygenation and Worse Neurological Outcome After Cardiac Arrest?Dokumen8 halamanIs Venous Congestion Associated With Reduced Cerebral Oxygenation and Worse Neurological Outcome After Cardiac Arrest?Anonymous ORleRrBelum ada peringkat
- Basics of Mechanical VentilationDokumen208 halamanBasics of Mechanical VentilationAnonymous ORleRr100% (1)
- Prokalsitonin Dan Kultur Darah Sebagai Penanda Sepsis Di Rsup DR Wahidin Sudirohusodo MakassarDokumen11 halamanProkalsitonin Dan Kultur Darah Sebagai Penanda Sepsis Di Rsup DR Wahidin Sudirohusodo MakassarAnonymous ORleRrBelum ada peringkat
- The Dog As An Animal Model For Intervertebral Disc Degeneration?Dokumen9 halamanThe Dog As An Animal Model For Intervertebral Disc Degeneration?Anonymous ORleRrBelum ada peringkat
- OA 737-11-18 Comparison Between Effectiveness of Transtracheal Block Alone Versus Superior Laryngeal1Dokumen5 halamanOA 737-11-18 Comparison Between Effectiveness of Transtracheal Block Alone Versus Superior Laryngeal1Anonymous ORleRrBelum ada peringkat
- ID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFDokumen10 halamanID Hubungan Faktor Resiko Dengan Terjadinya Nyeri Punggung Bawah Low Back Pain Pada PDFAnonymous aH8gCZ7zjBelum ada peringkat
- Management of Anembryonic Pregnancy Loss: An Observational StudyDokumen6 halamanManagement of Anembryonic Pregnancy Loss: An Observational StudyAnonymous ORleRrBelum ada peringkat
- Trends in Anaesthesia and Critical Care: Jamie Sleigh, Martyn Harvey, Logan Voss, Bill DennyDokumen6 halamanTrends in Anaesthesia and Critical Care: Jamie Sleigh, Martyn Harvey, Logan Voss, Bill DennyAnonymous ORleRrBelum ada peringkat
- International Journal of Infectious Diseases: SciencedirectDokumen4 halamanInternational Journal of Infectious Diseases: SciencedirectAnonymous ORleRrBelum ada peringkat
- OK Sio 2017Dokumen6 halamanOK Sio 2017Anonymous ORleRrBelum ada peringkat
- Felsenstein 2020Dokumen13 halamanFelsenstein 2020Mochamad RizkiBelum ada peringkat
- Acute Postoperative Pain at Rest After Hip and Knee Arthroplasty: Severity, Sensory Qualities and Impact On SleepDokumen6 halamanAcute Postoperative Pain at Rest After Hip and Knee Arthroplasty: Severity, Sensory Qualities and Impact On SleepAnonymous ORleRrBelum ada peringkat
- Gland Corporate BrochureDokumen6 halamanGland Corporate BrochureAnonymous ORleRrBelum ada peringkat
- Fluid Challenge Algorithm - 2006Dokumen1 halamanFluid Challenge Algorithm - 2006Anonymous ORleRrBelum ada peringkat
- Back Facts 10102Dokumen2 halamanBack Facts 10102Anonymous ORleRrBelum ada peringkat
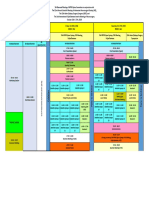
- UNAIR, ASAD, Surabaya Sanglah Hospital, Bali BNDCC, Bali BNDCC, BaliDokumen1 halamanUNAIR, ASAD, Surabaya Sanglah Hospital, Bali BNDCC, Bali BNDCC, BaliAnonymous ORleRrBelum ada peringkat
- Cover Dalam Dan Abstrak Siti Aisya Sakinah Web PDFDokumen3 halamanCover Dalam Dan Abstrak Siti Aisya Sakinah Web PDFAnonymous ORleRrBelum ada peringkat
- 605 FullDokumen3 halaman605 FullAnonymous ORleRrBelum ada peringkat
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDokumen3 halamanDiabetes & Metabolic Syndrome: Clinical Research & ReviewsAnonymous ORleRrBelum ada peringkat
- Algo ArrestDokumen2 halamanAlgo ArrestLocomotorica FK UkiBelum ada peringkat
- Annals of EpidemiologyDokumen7 halamanAnnals of EpidemiologyAnonymous ORleRrBelum ada peringkat
- Science of The Total Environment: Contents Lists Available atDokumen8 halamanScience of The Total Environment: Contents Lists Available atAnonymous ORleRrBelum ada peringkat
- Nautic Us Privacy PolicyDokumen3 halamanNautic Us Privacy PolicyAnonymous ORleRrBelum ada peringkat
- BJH 14482Dokumen12 halamanBJH 14482Anonymous ORleRrBelum ada peringkat
- BJH 14482Dokumen12 halamanBJH 14482Anonymous ORleRrBelum ada peringkat
- Perioperative Management of Thyroid DysfunctionDokumen5 halamanPerioperative Management of Thyroid DysfunctionAnonymous ORleRrBelum ada peringkat
- How To Verify Your Mobile NumberDokumen2 halamanHow To Verify Your Mobile NumberAnonymous ORleRrBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Anaphy Topic 3 IntegralDokumen3 halamanAnaphy Topic 3 Integral박제라Belum ada peringkat
- Management Accounting Tutorial QuestionsDokumen2 halamanManagement Accounting Tutorial Questionskanasai1992Belum ada peringkat
- Instant Download Learning Radiology e Book Recognizing The Basics 4th Edition With Audio Video Ebook PDF PDF FREEDokumen33 halamanInstant Download Learning Radiology e Book Recognizing The Basics 4th Edition With Audio Video Ebook PDF PDF FREEjane.mancini128100% (45)
- 2023 CBSE I Succeed Eng. Lang. Lit. K. A. Zone Poetry SectionDokumen9 halaman2023 CBSE I Succeed Eng. Lang. Lit. K. A. Zone Poetry SectioniCOS iSpace100% (1)
- McClain File WMDokumen10 halamanMcClain File WMthe kingfishBelum ada peringkat
- Development of Pharyngeal Arches 2Dokumen3 halamanDevelopment of Pharyngeal Arches 2NewtonBelum ada peringkat
- Room On The BroomDokumen31 halamanRoom On The BroomHebing WuBelum ada peringkat
- UJIAN SEMESTER GENAP B. Ing IXDokumen3 halamanUJIAN SEMESTER GENAP B. Ing IXMasdalyla TinendungBelum ada peringkat
- W2 Day 1 Belling The CatDokumen23 halamanW2 Day 1 Belling The Catgina domingoBelum ada peringkat
- 2ND Quarter Quiz 1 With Tos All Subjects New NormalDokumen15 halaman2ND Quarter Quiz 1 With Tos All Subjects New NormalEva G. AgarraBelum ada peringkat
- Read The Story. Answer The Questions That FollowDokumen1 halamanRead The Story. Answer The Questions That FollowRowena Casonete Dela TorreBelum ada peringkat
- Dodington 2018 Companion Species WantedDokumen3 halamanDodington 2018 Companion Species WantedAnna ConrickBelum ada peringkat
- Sanur WeeklyDokumen56 halamanSanur WeeklyGuz NusadaBelum ada peringkat
- A Guide To Out of The AbyssDokumen38 halamanA Guide To Out of The AbyssÇınar Atilla100% (1)
- GHOP Menu 2012 2 24Dokumen2 halamanGHOP Menu 2012 2 24administrator8147Belum ada peringkat
- Stepeni OvnaDokumen6 halamanStepeni OvnaTara SavicBelum ada peringkat
- False: Siempre Es Fácil Tener Una MascotaDokumen3 halamanFalse: Siempre Es Fácil Tener Una MascotaItzel López EugenioBelum ada peringkat
- Second Cot Science SixDokumen5 halamanSecond Cot Science Sixmaricel isletaBelum ada peringkat
- Knowledge Attitude and Practices of Oral Hygiene ADokumen5 halamanKnowledge Attitude and Practices of Oral Hygiene APatrycia Solavide SijabatBelum ada peringkat
- Evil DruidDokumen6 halamanEvil DruidkyryahnBelum ada peringkat
- Application of Proper DrapingDokumen15 halamanApplication of Proper DrapingCharls John Ercillo67% (6)
- Biology Quick Notes by Disha PublicationDokumen27 halamanBiology Quick Notes by Disha PublicationMunish Mechie100% (1)
- Applicator Manual - Phostoxin & PelletsDokumen43 halamanApplicator Manual - Phostoxin & PelletsZulfiqar AliBelum ada peringkat
- My Little PonyDokumen30 halamanMy Little PonyLady-Valerie TanBelum ada peringkat
- San Mar Kennel Inspection 060319eDokumen4 halamanSan Mar Kennel Inspection 060319eJustin DuncanBelum ada peringkat
- Mrs Bixby and The Colonel S CoatDokumen9 halamanMrs Bixby and The Colonel S CoatHst GonzalesBelum ada peringkat
- Anatomy DuodenumDokumen19 halamanAnatomy Duodenumzakardi nadalBelum ada peringkat
- NEC 11th Five Year Plan 2007-2011Dokumen109 halamanNEC 11th Five Year Plan 2007-2011Kamzalian Tomging100% (3)
- Eng-B w10 InternetDokumen6 halamanEng-B w10 InternetmoralassBelum ada peringkat
- CDC - Rabies Around The World - RabiesDokumen1 halamanCDC - Rabies Around The World - RabieskaminiBelum ada peringkat