Anda mungkin juga menyukai
- Wound Care Management 1Dokumen99 halamanWound Care Management 1Jan Oliver YaresBelum ada peringkat
- EarthingDokumen8 halamanEarthingDiana Filipe Travado Amaral100% (3)
- Assessing and Preventing Pressure UlcersDokumen8 halamanAssessing and Preventing Pressure UlcersTamil VillardoBelum ada peringkat
- Plasma Pen PDF Slidedeck 1Dokumen39 halamanPlasma Pen PDF Slidedeck 172034430Belum ada peringkat
- Dressing BedsoreDokumen66 halamanDressing BedsoreGirish Waru100% (1)
- Role Master FRP - HealingDokumen14 halamanRole Master FRP - HealingWayne GardnerBelum ada peringkat
- S M D U: KIN Anagement Ecubitis LcerDokumen77 halamanS M D U: KIN Anagement Ecubitis LcerabidBelum ada peringkat
- "PASS" Principles For Predictable PDFDokumen10 halaman"PASS" Principles For Predictable PDFkishan bordaBelum ada peringkat
- Health Teaching PlanDokumen3 halamanHealth Teaching PlanSammy Jr FamilarBelum ada peringkat
- Risk For Impaired Skin IntegrityDokumen4 halamanRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Kinesiology Taping Redefined (PDFDrive)Dokumen172 halamanKinesiology Taping Redefined (PDFDrive)Pahonțu Oana - ElenaBelum ada peringkat
- Wound CareDokumen14 halamanWound CareKirsten Padilla Chua100% (4)
- NURSING Case StudyDokumen14 halamanNURSING Case Studymuhammad fiaz50% (2)
- Final Coaching - PLE Surgery 2022Dokumen8 halamanFinal Coaching - PLE Surgery 2022JHON PAULO LAYUGBelum ada peringkat
- Pressure UlcerDokumen35 halamanPressure Ulcerenam professor100% (1)
- Wound CareDokumen7 halamanWound CareAbogadie Dione Blas ReyBelum ada peringkat
- DR - Monobina Sarker (Moic, Ccu) : Howrah District HospitalDokumen56 halamanDR - Monobina Sarker (Moic, Ccu) : Howrah District HospitalDeepa BhattacharjeeBelum ada peringkat
- Decubetic Ulcer (Bed Sores)Dokumen22 halamanDecubetic Ulcer (Bed Sores)Jerry ZahidBelum ada peringkat
- Guided Bone Regeneration ProcedureDokumen16 halamanGuided Bone Regeneration ProcedureAymen Elatrash100% (4)
- 3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsDokumen12 halaman3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsJOSHUA DICHOSOBelum ada peringkat
- Principles of Skin Care: A Guide for Nurses and Health Care PractitionersDari EverandPrinciples of Skin Care: A Guide for Nurses and Health Care PractitionersBelum ada peringkat
- Hand BurnDokumen57 halamanHand BurnjoismdBelum ada peringkat
- FACIAL CUPPING TECHNIQUES: Learn To Do at HomeDari EverandFACIAL CUPPING TECHNIQUES: Learn To Do at HomePenilaian: 4 dari 5 bintang4/5 (1)
- Aim4aiims - In: Pathology Board ExaminationDokumen72 halamanAim4aiims - In: Pathology Board ExaminationdorjeesengeBelum ada peringkat
- ANSWER KEY 1-39Dokumen78 halamanANSWER KEY 1-39Nicomille T. Caliging80% (5)
- Wound HealingDokumen62 halamanWound HealingRisPerdanaBelum ada peringkat
- NCP - Impaired Skin IntegrityDokumen3 halamanNCP - Impaired Skin IntegrityFlauros Ryu Jabien90% (29)
- Unit 11 Skin Integrity and Wound CareDokumen47 halamanUnit 11 Skin Integrity and Wound CareAshaBelum ada peringkat
- Periodontal Flap Design and HealingDokumen93 halamanPeriodontal Flap Design and HealingRaghavendra NaikBelum ada peringkat
- Pressure Ulcer Prevention & Management: Wocare ClinicDokumen20 halamanPressure Ulcer Prevention & Management: Wocare ClinicShoahir RustanBelum ada peringkat
- Pressure Ulcers: by Mr. M. Shivanandha ReddyDokumen35 halamanPressure Ulcers: by Mr. M. Shivanandha ReddyDr Ali100% (2)
- Decubitus UlcersDokumen4 halamanDecubitus UlcersNkk Aqnd MgdnglBelum ada peringkat
- W2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsDokumen6 halamanW2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsKyla L. Madjad100% (1)
- NCP CVDDokumen5 halamanNCP CVDaejel1889% (9)
- German New Medicine Therapy: A Brief SummaryDokumen5 halamanGerman New Medicine Therapy: A Brief Summaryiristv irisBelum ada peringkat
- Skin Sense!: A Dermatologist's Guide to Skin and Facial Care; Third EditionDari EverandSkin Sense!: A Dermatologist's Guide to Skin and Facial Care; Third EditionPenilaian: 5 dari 5 bintang5/5 (12)
- NCP Impaired Skin IntergrityDokumen3 halamanNCP Impaired Skin IntergrityGrape JuiceBelum ada peringkat
- Pressure Ulcer Prevention: Tips for Reducing RiskDokumen15 halamanPressure Ulcer Prevention: Tips for Reducing RiskRajaRafianBelum ada peringkat
- Pressure Ulcer.... by MoumitDokumen4 halamanPressure Ulcer.... by MoumitMoumita MandalBelum ada peringkat
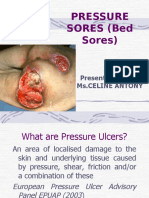
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDokumen40 halamanPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiBelum ada peringkat
- Bedsores: Eligrace F. Fabian, RNDokumen22 halamanBedsores: Eligrace F. Fabian, RNsweetsai05Belum ada peringkat
- Pressure Sores 3Dokumen39 halamanPressure Sores 3zahraaBelum ada peringkat
- Pressure Ulcer DR MirfatDokumen50 halamanPressure Ulcer DR MirfatDrmirfat AlkashifBelum ada peringkat
- Support SurfacesDokumen4 halamanSupport SurfacesKennard Aristo ArifinBelum ada peringkat
- Pressure Ulcer DR MirfatDokumen50 halamanPressure Ulcer DR MirfatDrmirfat AlkashifBelum ada peringkat
- 1.RagragPreventing Pressure Sore.1Dokumen18 halaman1.RagragPreventing Pressure Sore.1alsamixersBelum ada peringkat
- Nurses Role in Care & Prevention of PressureDokumen25 halamanNurses Role in Care & Prevention of PressureLinda andayaniBelum ada peringkat
- PHYSICAL REHABILITATION GUIDEDokumen9 halamanPHYSICAL REHABILITATION GUIDEEvan Permana PutraBelum ada peringkat
- Gen Med Study GuideDokumen21 halamanGen Med Study GuideHannahBennieBelum ada peringkat
- Physical Properties of Skin and Its ApplicationsDokumen94 halamanPhysical Properties of Skin and Its ApplicationsdrshilpibhadaniBelum ada peringkat
- La UlcersDokumen3 halamanLa Ulcersas3d_laoBelum ada peringkat
- NANDA Definition:: Ongoing AssessmentDokumen3 halamanNANDA Definition:: Ongoing AssessmentKat LazoBelum ada peringkat
- General Guidelines For Skin CareDokumen4 halamanGeneral Guidelines For Skin CareDaesungBelum ada peringkat
- DAY 2 Mahesa Burn Rehabilitation PresentasiDokumen16 halamanDAY 2 Mahesa Burn Rehabilitation Presentasichristin megaBelum ada peringkat
- Back CareDokumen56 halamanBack CareSandeep Maan100% (2)
- Pressure Ulcers Hand OutDokumen52 halamanPressure Ulcers Hand OutAdiAri RosiuBelum ada peringkat
- Skin and Pressure SoresDokumen24 halamanSkin and Pressure SoresJennyBelum ada peringkat
- Preventing Skin Breakdown and Promoting NutritionDokumen2 halamanPreventing Skin Breakdown and Promoting NutritionJohn Ford VisoriaBelum ada peringkat
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG Independent STDokumen4 halamanAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: STG Independent STFrando kennethBelum ada peringkat
- ASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONDokumen4 halamanASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONArian May MarcosBelum ada peringkat
- Skin IntegrityDokumen112 halamanSkin IntegrityHerlina NababanBelum ada peringkat
- Bedsores PDFDokumen13 halamanBedsores PDFsimi yBelum ada peringkat
- Skin Care and Management of Pressure UlcerDokumen24 halamanSkin Care and Management of Pressure UlcerchellczyBelum ada peringkat
- Decubitis Ulcer Prevention and TreatmentDokumen21 halamanDecubitis Ulcer Prevention and TreatmentWIKKI vinesBelum ada peringkat
- NCP 3Dokumen3 halamanNCP 3hsiriaBelum ada peringkat
- Integu11 Pressure UlcresDokumen11 halamanIntegu11 Pressure UlcresEliza ButtBelum ada peringkat
- SJMC - xi-nCP&HTP - Impaired Skin IntegrityDokumen10 halamanSJMC - xi-nCP&HTP - Impaired Skin IntegrityJoy CompetenteBelum ada peringkat
- Burn InjuryDokumen80 halamanBurn InjuryQueena Neysa CalcarinaBelum ada peringkat
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDokumen7 halamanPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoBelum ada peringkat
- Soft Tissue Healing After Different Flap Designs in Periapical SurgeryDokumen4 halamanSoft Tissue Healing After Different Flap Designs in Periapical SurgeryallthewayhomeBelum ada peringkat
- Ms. Jocelyn BautistaDokumen2 halamanMs. Jocelyn BautistaMela VincoBelum ada peringkat
- Geistlich Bio-Oss Collagen and Geistlich Bio-Gide in Extraction SocketsDokumen6 halamanGeistlich Bio-Oss Collagen and Geistlich Bio-Gide in Extraction SocketsErdeli StefaniaBelum ada peringkat
- Effect of Low-Level Laser Therapy On Bone Repair Histological Study in RatsDokumen9 halamanEffect of Low-Level Laser Therapy On Bone Repair Histological Study in RatsPé KhìnBelum ada peringkat
- Henna, Lawsonia Inermis1Dokumen28 halamanHenna, Lawsonia Inermis1zaheeda1984Belum ada peringkat
- Ash As A Healing MediatorDokumen7 halamanAsh As A Healing MediatoriajpsBelum ada peringkat
- Healing and Keeping Prayer (2013)Dokumen2 halamanHealing and Keeping Prayer (2013)Kylie DanielsBelum ada peringkat
- Swimmers ShoulderDokumen26 halamanSwimmers ShoulderThunder CrackerBelum ada peringkat
- Pathophysiology Chapter 3 SummaryDokumen8 halamanPathophysiology Chapter 3 SummaryMcat NotensionBelum ada peringkat
- Unit 1 - Pp. 4-7: Flash On English For NURSING Answer Key and TranscriptsDokumen25 halamanUnit 1 - Pp. 4-7: Flash On English For NURSING Answer Key and TranscriptsMarla PeppersBelum ada peringkat
- Fapc-Chapter-2-Wound HealingDokumen6 halamanFapc-Chapter-2-Wound HealingMiñoza, Aeris GabrielleBelum ada peringkat
- HEALTH TEACHING PLAN FOR WOUND CAREDokumen4 halamanHEALTH TEACHING PLAN FOR WOUND CAREAsterlyn ConiendoBelum ada peringkat
- Wound and Wound Dressing Dressing: Presentedby Mrs - Sylvia Ranjan Mathew Principal MGM College of NursingDokumen21 halamanWound and Wound Dressing Dressing: Presentedby Mrs - Sylvia Ranjan Mathew Principal MGM College of Nursingjyoti singhBelum ada peringkat
- The Dry Fasting Miracle From Deprive To Thrive (Luke Coutinho Sheikh Abdul Aziz Nuaimi) (Z-Library)Dokumen184 halamanThe Dry Fasting Miracle From Deprive To Thrive (Luke Coutinho Sheikh Abdul Aziz Nuaimi) (Z-Library)ryarok1Belum ada peringkat
- Gingival Surgical TechniquesDokumen88 halamanGingival Surgical TechniquesDr. Debbie SabladaBelum ada peringkat
- Cameron 1995Dokumen7 halamanCameron 1995Seno SenyBelum ada peringkat
- Ue Gen PathologyDokumen287 halamanUe Gen PathologyReza RastgooBelum ada peringkat
- Acephalous MouthDokumen8 halamanAcephalous Mouthdelinkuent100% (1)
- Otoplasty - CairnsDokumen12 halamanOtoplasty - CairnsLaineyBelum ada peringkat