Anda mungkin juga menyukai
- PLL Frequency Control For Ultrasonic GeneratorsDokumen2 halamanPLL Frequency Control For Ultrasonic Generatorsapi-3809613Belum ada peringkat
- Tools of Micro & Nano FabricationDokumen39 halamanTools of Micro & Nano Fabricationkaushik4208100% (2)
- Nano Technology: Utkal UniversityDokumen33 halamanNano Technology: Utkal UniversityShradha SubhadarshineeBelum ada peringkat
- HST 362 Sources 2011 PDFDokumen27 halamanHST 362 Sources 2011 PDFLéo LacerdaBelum ada peringkat
- Design and Analysis of Ultrasonic Horns Operating in Longitudinal and Torsional VibrationDokumen178 halamanDesign and Analysis of Ultrasonic Horns Operating in Longitudinal and Torsional VibrationkumargpalaniBelum ada peringkat
- Gas LasersDokumen4 halamanGas LasersPayal SinghalBelum ada peringkat
- Preventive HealthDokumen380 halamanPreventive HealthmurappanadBelum ada peringkat
- Strahlenfolter - Ultrasonic DevicesDokumen5 halamanStrahlenfolter - Ultrasonic Devicesstop-nwo-nazi-folter100% (1)
- Additive Manufacturing Using Selective Electron Beam MeltingDokumen8 halamanAdditive Manufacturing Using Selective Electron Beam MeltingHiki ChannelBelum ada peringkat
- CRT InformationDokumen5 halamanCRT InformationA CBelum ada peringkat
- LaserDokumen21 halamanLaserJisha Mariam JoseBelum ada peringkat
- CST Charged Particle Simulation LowDokumen2 halamanCST Charged Particle Simulation Low9999igi100% (1)
- 4936-Assist Gas Flow Chart For LasersDokumen1 halaman4936-Assist Gas Flow Chart For LasersMinh Nguyen TuanBelum ada peringkat
- Three-Dimensional Sound Source Localization UsingDokumen15 halamanThree-Dimensional Sound Source Localization UsingWill D'Andrea FonsecaBelum ada peringkat
- Colloidal Silver, Scarlet Fever and Streptococcus Pyogenes - A New Plague Begins To SpreadDokumen8 halamanColloidal Silver, Scarlet Fever and Streptococcus Pyogenes - A New Plague Begins To SpreaddropsyBelum ada peringkat
- X-Ray Production and Factors Controlling X Ray BeamsDokumen14 halamanX-Ray Production and Factors Controlling X Ray Beamsankur sharma100% (1)
- Efficient Small-Scale Gold Mining: The Long Tom SluiceDokumen6 halamanEfficient Small-Scale Gold Mining: The Long Tom SluiceJovanny HerreraBelum ada peringkat
- Electricity Basics: Charges, Fields and CurrentsDokumen17 halamanElectricity Basics: Charges, Fields and CurrentsAyushJaiswalBelum ada peringkat
- A Uri Culo TherapyDokumen22 halamanA Uri Culo TherapySubramanya SeshagiriBelum ada peringkat
- The Right Way To Do Wrong PDFDokumen117 halamanThe Right Way To Do Wrong PDFNisic222Belum ada peringkat
- A Future Perspective For Regenerative Medicine - Understanding The Concept of Vibrational MedicineDokumen12 halamanA Future Perspective For Regenerative Medicine - Understanding The Concept of Vibrational MedicineDan TudorBelum ada peringkat
- Alexander BainDokumen6 halamanAlexander BainNur HaBelum ada peringkat
- Goodnews Re Nuclear DestructionDokumen4 halamanGoodnews Re Nuclear DestructionshorinjinBelum ada peringkat
- Barrett's OesophagusDokumen20 halamanBarrett's OesophagusArri KurniawanBelum ada peringkat
- Python For SeismologyDokumen4 halamanPython For SeismologyKanita Nur IzzatiBelum ada peringkat
- Chapter 1 The First HumansDokumen72 halamanChapter 1 The First HumansDavid Duez100% (1)
- Colloidal Silver - US Space StationDokumen2 halamanColloidal Silver - US Space Stationscottc9Belum ada peringkat
- 06 Boston Ear Maps Orthopaedic Organ Heart Web PDFDokumen8 halaman06 Boston Ear Maps Orthopaedic Organ Heart Web PDFYouvanoBelum ada peringkat
- Disk Management From The Command-Line, Part 1 - The InstructionalDokumen10 halamanDisk Management From The Command-Line, Part 1 - The Instructionalscribd-123Belum ada peringkat
- Fender Princeton 65 DSPDokumen8 halamanFender Princeton 65 DSPMiniEscortBelum ada peringkat
- Bio Disc IntroDokumen19 halamanBio Disc IntroBrako Jones100% (1)
- MicroReview-Small Molecules That Regulate Lifespan-Evidence For XenohormesisDokumen7 halamanMicroReview-Small Molecules That Regulate Lifespan-Evidence For Xenohormesismarijana_zBelum ada peringkat
- Nanotechnology in Processors and Nokia MorphDokumen36 halamanNanotechnology in Processors and Nokia MorphAvinash SinghBelum ada peringkat
- Clin Anat 07 Spinal Segmental Bone InnervationDokumen5 halamanClin Anat 07 Spinal Segmental Bone InnervationOchiMataBelum ada peringkat
- Ivermectin As A Potential Therapeutic Agent For COVID-19-CasestudiesDokumen3 halamanIvermectin As A Potential Therapeutic Agent For COVID-19-CasestudiesMilly Farisa KurniaBelum ada peringkat
- Expert Reveals How to Best Protect From EMFs and 5GDokumen44 halamanExpert Reveals How to Best Protect From EMFs and 5GgoguBelum ada peringkat
- Necessity of Transmission & DistributionDokumen80 halamanNecessity of Transmission & DistributionveenadivyakishBelum ada peringkat
- Scabies-2017-The Journal of DermatologyDokumen24 halamanScabies-2017-The Journal of DermatologysirohBelum ada peringkat
- Risk Mobile Phones 05Dokumen16 halamanRisk Mobile Phones 05Chandan GuptaBelum ada peringkat
- Small Molecule Activators of Sirtuins Extend Saccharomyces Cerevisiae LifespanDokumen5 halamanSmall Molecule Activators of Sirtuins Extend Saccharomyces Cerevisiae LifespanMiguel Angel Salazar SánchezBelum ada peringkat
- 2020 Wddty February 2020Dokumen84 halaman2020 Wddty February 2020San RajBelum ada peringkat
- Beneficial, Normalizing', and Stimulating FrequenciesDokumen3 halamanBeneficial, Normalizing', and Stimulating FrequenciesAndre MaratteusBelum ada peringkat
- How Voltage, Current, Time and Path Affect Electric Shock SeverityDokumen21 halamanHow Voltage, Current, Time and Path Affect Electric Shock SeverityHeidi RiegoBelum ada peringkat
- Electrical Stimulation at AuricularDokumen9 halamanElectrical Stimulation at AuricularshaukijameelBelum ada peringkat
- Finishing Essentials: Technique CollectionDokumen12 halamanFinishing Essentials: Technique CollectionNGAMIJEBelum ada peringkat
- Etc GunDokumen30 halamanEtc GunjobseekeramatxBelum ada peringkat
- Solar Energy 2008Dokumen58 halamanSolar Energy 2008Prakash VenkatesanBelum ada peringkat
- Sources of Intracellular OsmolarityDokumen1 halamanSources of Intracellular OsmolarityJohnBelum ada peringkat
- Introduction - 2017 - Rhythmic Stimulation Procedures in Neuromodulation PDFDokumen6 halamanIntroduction - 2017 - Rhythmic Stimulation Procedures in Neuromodulation PDFGeo MeBelum ada peringkat
- High Frequency Currents Frederich Finch Strong 1908 Arvhive Org PDFDokumen320 halamanHigh Frequency Currents Frederich Finch Strong 1908 Arvhive Org PDFsweetohmBelum ada peringkat
- Cape Town's Amazing Network of Nature ReservesDokumen45 halamanCape Town's Amazing Network of Nature ReserveswinstonBelum ada peringkat
- 2011 Consumer Residential PDFDokumen27 halaman2011 Consumer Residential PDFKeiko JeyaBelum ada peringkat
- Total Phenolic Content and Antioxydant Activity of Two Rhododendron Species Collected From The Rize Province (Turkey)Dokumen6 halamanTotal Phenolic Content and Antioxydant Activity of Two Rhododendron Species Collected From The Rize Province (Turkey)Premier Publishers100% (1)
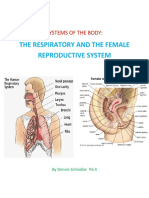
- Systems of The BodyDokumen10 halamanSystems of The BodyKatrina SchindlarBelum ada peringkat
- The World Tomorrow - Sample Anti Imperialist Edition - Feb 1927Dokumen48 halamanThe World Tomorrow - Sample Anti Imperialist Edition - Feb 1927Michael ThompsonBelum ada peringkat
- Complex Oscillatory Waves Emerging From Cortical Organoids Model Early Human Brain Network DevelopmentDokumen20 halamanComplex Oscillatory Waves Emerging From Cortical Organoids Model Early Human Brain Network DevelopmentThePoliticalHatBelum ada peringkat
- Thermoplastics and ThermosetsDokumen21 halamanThermoplastics and ThermosetsNasmin BasheerBelum ada peringkat
- Atlas of Orthodontics - ViazisDokumen320 halamanAtlas of Orthodontics - ViazisAdil Houem100% (20)
- Clear Aligner Therapy in The Mixed Dentition - Indications and PraDokumen51 halamanClear Aligner Therapy in The Mixed Dentition - Indications and Pra黎燦燦Belum ada peringkat
- Diaphragm Vacuum Pumps For Autoclaves: Concept Areas of Use FeaturesDokumen5 halamanDiaphragm Vacuum Pumps For Autoclaves: Concept Areas of Use Featuresnotaden1849Belum ada peringkat
- DOwnoad 1Dokumen21 halamanDOwnoad 1Ahmad Zaidi100% (2)
- Advance Brochure UKDokumen6 halamanAdvance Brochure UKnotaden1849Belum ada peringkat
- Vacuum Pumps For Table Top Steam Autoclaves: Application BrochureDokumen8 halamanVacuum Pumps For Table Top Steam Autoclaves: Application Brochurenotaden1849Belum ada peringkat
- Av/L & Av/S: VES - Steam Sterilizing AutoclavesDokumen6 halamanAv/L & Av/S: VES - Steam Sterilizing Autoclavesnotaden1849Belum ada peringkat
- 7000 Distiller ManualDokumen12 halaman7000 Distiller ManualvicdiaBelum ada peringkat
- Unfire Pressure VesselDokumen146 halamanUnfire Pressure Vesselsungkang83% (6)
- Notaden Scania B Scan PDFDokumen2 halamanNotaden Scania B Scan PDFnotaden1849Belum ada peringkat
- Hospital Management System Mamcet 2008itDokumen10 halamanHospital Management System Mamcet 2008itmatt uyeBelum ada peringkat
- Zomato Annual ReportDokumen13 halamanZomato Annual Reportnotaden1849Belum ada peringkat
- Perimetry Brochure US PER4622 REVB 2014Dokumen14 halamanPerimetry Brochure US PER4622 REVB 2014notaden1849Belum ada peringkat
- Fifo InformationDokumen14 halamanFifo Informationnotaden1849Belum ada peringkat
- Introducción Al AutoclaveDokumen7 halamanIntroducción Al Autoclaverafcat1974Belum ada peringkat
- HE359RTD100Dokumen3 halamanHE359RTD100notaden1849Belum ada peringkat
- CP2 TemperatureDokumen22 halamanCP2 TemperatureAilton De Sousa GonçalvesBelum ada peringkat
- Systec D 45 enDokumen1 halamanSystec D 45 ennotaden1849Belum ada peringkat
- MERLIN® Surgical System: A Halma Company A Halma CompanyDokumen4 halamanMERLIN® Surgical System: A Halma Company A Halma Companynotaden1849Belum ada peringkat
- Interfacing The TLC5510 Analog To Digital Converter To The TMS320C203 DSPDokumen22 halamanInterfacing The TLC5510 Analog To Digital Converter To The TMS320C203 DSPnotaden1849Belum ada peringkat
- Rec3-S DRDokumen2 halamanRec3-S DRnotaden1849Belum ada peringkat
- VNA Flyer IFA InterfaceDokumen2 halamanVNA Flyer IFA Interfacenotaden1849Belum ada peringkat
- Notaden Scania B ScanDokumen2 halamanNotaden Scania B Scannotaden1849Belum ada peringkat
- Small SterilizerDokumen36 halamanSmall Sterilizernotaden1849100% (1)
- Piezo ScalarDokumen6 halamanPiezo Scalarnotaden1849Belum ada peringkat
- Bi OmegaDokumen14 halamanBi Omeganotaden1849Belum ada peringkat
- TT Automatic LineDokumen8 halamanTT Automatic Linenotaden1849Belum ada peringkat
- Statim 5.1 Field Troubleshooting Guide PDFDokumen59 halamanStatim 5.1 Field Troubleshooting Guide PDFLeandro Neves de Oliveira100% (1)
- Piezo Scalar1Dokumen9 halamanPiezo Scalar1notaden1849Belum ada peringkat
- XT Series CPAP BrochureDokumen8 halamanXT Series CPAP Brochurenotaden1849Belum ada peringkat
- TINGET ClassB AutoclavesDokumen4 halamanTINGET ClassB Autoclavesnotaden1849Belum ada peringkat
- Propaganda AssignmentDokumen3 halamanPropaganda Assignmentapi-653920203Belum ada peringkat
- Crane's Manual - CV ValuesDokumen14 halamanCrane's Manual - CV Valuesnghiemta18Belum ada peringkat
- Grade 5 DLL SCIENCE 5 Q4 Week 9Dokumen6 halamanGrade 5 DLL SCIENCE 5 Q4 Week 9Joanna Marie Cruz FelipeBelum ada peringkat
- The Bare Foot Boy 3 Ab 2 ManadoDokumen100 halamanThe Bare Foot Boy 3 Ab 2 ManadoKotakuBelum ada peringkat
- QP ScriptDokumen57 halamanQP ScriptRitesh SharmaBelum ada peringkat
- Week #7 - CH #9 - Employee Empowerment and Interpersonal InterventionsDokumen37 halamanWeek #7 - CH #9 - Employee Empowerment and Interpersonal InterventionsAhmed TahirBelum ada peringkat
- PGW Spring SuitDokumen14 halamanPGW Spring Suitapi-3700386Belum ada peringkat
- Dr. Sun Chemistry Summary 2019 PDFDokumen75 halamanDr. Sun Chemistry Summary 2019 PDFPranav ChatiBelum ada peringkat
- LESSON 1.1.2 - Online PlatformsDokumen5 halamanLESSON 1.1.2 - Online PlatformsAndree Laxamana100% (1)
- Design Audit ToolDokumen7 halamanDesign Audit ToolThe Dementia Centre100% (1)
- NCLT Orders Relief To Home BuyersDokumen7 halamanNCLT Orders Relief To Home BuyersPGurusBelum ada peringkat
- Physics EducationDokumen14 halamanPhysics Educationchrisuche100% (2)
- Gauteng Grade 6 Maths ExamDokumen14 halamanGauteng Grade 6 Maths ExamMolemo S MasemulaBelum ada peringkat
- Introduction To Pharmacy ManagementDokumen28 halamanIntroduction To Pharmacy ManagementSirry HidayaniBelum ada peringkat
- Paradine V Jane - (1646) 82 ER 897Dokumen2 halamanParadine V Jane - (1646) 82 ER 897TimishaBelum ada peringkat
- Hedge Fund Strategies, Mutual Fund Comparison & Fund of FundsDokumen46 halamanHedge Fund Strategies, Mutual Fund Comparison & Fund of Fundsbboyvn100% (1)
- ARGUMENTS AGAINST AND IN FAVOR OF THE DEATH PENALTYDokumen18 halamanARGUMENTS AGAINST AND IN FAVOR OF THE DEATH PENALTYRod Herrero PinoBelum ada peringkat
- A Course in KettlebellsDokumen40 halamanA Course in KettlebellsMagoots100% (1)
- Dendrinos, Multilingualism Language Policy in The EU TodayDokumen20 halamanDendrinos, Multilingualism Language Policy in The EU Todayi.giommettiBelum ada peringkat
- Pan AfricanismDokumen12 halamanPan AfricanismOscar MasindeBelum ada peringkat
- Baby Crawling - How Important Really It IsDokumen2 halamanBaby Crawling - How Important Really It Ismarkus_danusantosoBelum ada peringkat
- Balancing The Cybersecurity BattlefieldDokumen4 halamanBalancing The Cybersecurity BattlefieldLilminowBelum ada peringkat
- Cept To Cept Company PVT LTDDokumen17 halamanCept To Cept Company PVT LTDRatnil ShrivastavaBelum ada peringkat
- Somatic Symptom DisorderDokumen26 halamanSomatic Symptom DisorderGAYATHRI NARAYANAN100% (1)
- 1.7 The Lagrangian DerivativeDokumen6 halaman1.7 The Lagrangian DerivativedaskhagoBelum ada peringkat
- Violent Extremism in South AfricaDokumen20 halamanViolent Extremism in South AfricaMulidsahayaBelum ada peringkat
- THE QUALITY OF LITERARY ENGLISH VIETNAMESE TRANSLATIONS TODAY. LƯỜNG THỊ THÚY.QH.1.EDokumen64 halamanTHE QUALITY OF LITERARY ENGLISH VIETNAMESE TRANSLATIONS TODAY. LƯỜNG THỊ THÚY.QH.1.EKavic100% (2)
- Perspective in PharmacyDokumen3 halamanPerspective in PharmacyAgniez Hannah Permites100% (4)
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDokumen15 halamanCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarBelum ada peringkat