Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- (L) Examples of Machine Shop Practice (1910)Dokumen54 halaman(L) Examples of Machine Shop Practice (1910)Ismael 8877100% (1)
- 2011 Hyundai Service FiltersDokumen18 halaman2011 Hyundai Service FiltersTan JaiBelum ada peringkat
- HP Deskjet Printer Supply ChainDokumen19 halamanHP Deskjet Printer Supply ChainJose Barnon86% (7)
- Vandex CrystallineDokumen12 halamanVandex CrystallineJoseph ChenBelum ada peringkat
- Eco SPARDokumen3 halamanEco SPARMohammad LabinBelum ada peringkat
- P102 Lesson 4Dokumen24 halamanP102 Lesson 4Tracy Blair Napa-egBelum ada peringkat
- Food Safety and StandardsDokumen8 halamanFood Safety and StandardsArifSheriffBelum ada peringkat
- Business and Finance TerminologyDokumen15 halamanBusiness and Finance TerminologyKat KatBelum ada peringkat
- sb485s rs232 A rs485Dokumen24 halamansb485s rs232 A rs485KAYCONSYSTECSLA KAYLA CONTROL SYSTEMBelum ada peringkat
- Moot Problem FinalDokumen2 halamanMoot Problem FinalHimanshi SaraiyaBelum ada peringkat
- Amended Formal ComplaintDokumen87 halamanAmended Formal ComplaintWXYZ-TV Channel 7 DetroitBelum ada peringkat
- Tata Steel Ratio AnalysisDokumen41 halamanTata Steel Ratio AnalysisGourav VallakattiBelum ada peringkat
- Minimalist CV ResumeDokumen1 halamanMinimalist CV ResumeSijith MathewBelum ada peringkat
- Lower Gasket Kit (S/N E/ 9Fz999 & Below) : Model Number: 335 Serial Number: A9KA11001 & Above, AAD111001 & AboveDokumen2 halamanLower Gasket Kit (S/N E/ 9Fz999 & Below) : Model Number: 335 Serial Number: A9KA11001 & Above, AAD111001 & Abovezeeshan tanveerBelum ada peringkat
- Business Ethics Final Work Brief 2Dokumen6 halamanBusiness Ethics Final Work Brief 2KALIZA TRESSY MEGHANBelum ada peringkat
- Uniarch Network Video Recorders User Manual-V1.00Dokumen99 halamanUniarch Network Video Recorders User Manual-V1.00amurjiantoBelum ada peringkat
- Lesson Worksheet: 6.1A MeanDokumen7 halamanLesson Worksheet: 6.1A Meanwaiman fuBelum ada peringkat
- Intel Core - WikipediaDokumen16 halamanIntel Core - WikipediaEEBB0% (1)
- Clark Hess1Dokumen668 halamanClark Hess1Jeyner Chavez VasquezBelum ada peringkat
- HYD CCU: TICKET - ConfirmedDokumen2 halamanHYD CCU: TICKET - ConfirmedRahul ValapadasuBelum ada peringkat
- 2.1 Article On Reasonable Compensation Job Aid 4-15-2015Dokumen3 halaman2.1 Article On Reasonable Compensation Job Aid 4-15-2015Michael GregoryBelum ada peringkat
- OBLICONDokumen13 halamanOBLICONZARABelum ada peringkat
- 6 Elements of A Healthy ChurchDokumen2 halaman6 Elements of A Healthy ChurchJayhia Malaga JarlegaBelum ada peringkat
- ZPPF ChallanDokumen1 halamanZPPF ChallanGunasekhar ReddyBelum ada peringkat
- Lezione Argiolu - Master Roma3!3!12-2010 - Test Di Application SecurityDokumen26 halamanLezione Argiolu - Master Roma3!3!12-2010 - Test Di Application SecurityWB_YeatsBelum ada peringkat
- Vol II - PIM (Feasibility Report) For Resort at ChorwadDokumen42 halamanVol II - PIM (Feasibility Report) For Resort at Chorwadmyvin jovi denzilBelum ada peringkat
- Oil and Gas Reloaded: Offshore ArgentinaDokumen9 halamanOil and Gas Reloaded: Offshore ArgentinaMuhammad Fahmi AnbBelum ada peringkat
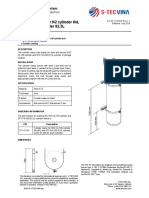
- Cylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LDokumen1 halamanCylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LNguyễn Minh ThiệuBelum ada peringkat
- 150 67-Eg1Dokumen104 halaman150 67-Eg1rikoBelum ada peringkat
- Technical Schedule World BankDokumen249 halamanTechnical Schedule World BankPramod ShastryBelum ada peringkat