Anda mungkin juga menyukai
- Complex Care Management Toolkit PDFDokumen14 halamanComplex Care Management Toolkit PDFumi khasanahBelum ada peringkat
- Drug Suffixes Cheat Sheet Sorted by Drug TypeDokumen3 halamanDrug Suffixes Cheat Sheet Sorted by Drug TypeJennaBelum ada peringkat
- The NHS in 2030 - A People-Powered and Knowledge-Powered Health SystemDokumen48 halamanThe NHS in 2030 - A People-Powered and Knowledge-Powered Health SystemNestaBelum ada peringkat
- Basic SeismicDokumen40 halamanBasic Seismiczeze_13Belum ada peringkat
- Sсiеntifiс Аmеricаn - 2020-12 PDFDokumen88 halamanSсiеntifiс Аmеricаn - 2020-12 PDFAlvaro Franco GonzalezBelum ada peringkat
- Pfizer PBC BookletDokumen7 halamanPfizer PBC BookletDon HeymannBelum ada peringkat
- Seismic ExplorDokumen45 halamanSeismic Explorzeze_13Belum ada peringkat
- Brach y TherapyDokumen3 halamanBrach y Therapydincy danielBelum ada peringkat
- Slicing Pie NotesDokumen57 halamanSlicing Pie Noteszeze_13100% (2)
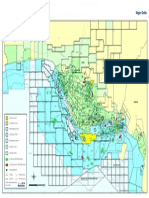
- Map of Nigeria Oil FieldDokumen1 halamanMap of Nigeria Oil Fieldriddi12355% (11)
- Innovation in HealthcareDokumen21 halamanInnovation in HealthcareFatima Khalid100% (1)
- Columbia Dental MagazineDokumen44 halamanColumbia Dental MagazineAegissBelum ada peringkat
- Sultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputDokumen5 halamanSultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputRAHIB SAMAYATINBelum ada peringkat
- Public Health AssignmentDokumen6 halamanPublic Health AssignmentGeorgia PooleBelum ada peringkat
- Precision Medicine OncologyDokumen18 halamanPrecision Medicine Oncologyaminudinrahman100% (1)
- A Solution Model For Stuck-Pipe & Fishing Challenges in Geothermal Drilling - A Case of The Olkaria Geothermal FieldDokumen9 halamanA Solution Model For Stuck-Pipe & Fishing Challenges in Geothermal Drilling - A Case of The Olkaria Geothermal Fieldzeze_13Belum ada peringkat
- ATK - Building Value-Based Healthcare Business ModelsDokumen11 halamanATK - Building Value-Based Healthcare Business Modelsapritul3539Belum ada peringkat
- Purchasing Medical Innovation: The Right Technology, for the Right Patient, at the Right PriceDari EverandPurchasing Medical Innovation: The Right Technology, for the Right Patient, at the Right PriceBelum ada peringkat
- Crohn's Disease Seminar FinalDokumen27 halamanCrohn's Disease Seminar Finalshahad alshareefBelum ada peringkat
- Covid WarriorsDokumen103 halamanCovid WarriorsMG Rao100% (1)
- Metabical CBDokumen31 halamanMetabical CBKumar AbhishekBelum ada peringkat
- Health informatics: Improving patient careDari EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITPenilaian: 3 dari 5 bintang3/5 (1)
- Project Report of International Hospital BanditaDokumen99 halamanProject Report of International Hospital Banditapolly1963Belum ada peringkat
- Hacking Healthcare: Designing Human-Centered Technology for a Healthier FutureDari EverandHacking Healthcare: Designing Human-Centered Technology for a Healthier FuturePenilaian: 4 dari 5 bintang4/5 (1)
- Benefits OfTelemedicineDokumen6 halamanBenefits OfTelemedicineMurangwa AlbertBelum ada peringkat
- Humanising Healthcare: Patterns of Hope for a System Under StrainDari EverandHumanising Healthcare: Patterns of Hope for a System Under StrainPenilaian: 5 dari 5 bintang5/5 (1)
- The Henry Fords of Healthcar: Lessons the West Can Learn from the EastDari EverandThe Henry Fords of Healthcar: Lessons the West Can Learn from the EastBelum ada peringkat
- Innovation Health and Wealth Report 2012dh - 134597Dokumen36 halamanInnovation Health and Wealth Report 2012dh - 134597Alejandro CardonaBelum ada peringkat
- Intelligent Kindness: Reforming The Culture of HealthcareDokumen7 halamanIntelligent Kindness: Reforming The Culture of Healthcarefarnaz_2647334Belum ada peringkat
- Nudge and Missed Apointments-2015Dokumen8 halamanNudge and Missed Apointments-2015cjbae22Belum ada peringkat
- Imelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandDokumen11 halamanImelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandhppnukBelum ada peringkat
- Tackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettDokumen15 halamanTackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettLesley Russell100% (1)
- 1980 Reith3Dokumen8 halaman1980 Reith3Sum LamBelum ada peringkat
- Healt (15384)Dokumen110 halamanHealt (15384)Oscar Javier Gaitan TrujilloBelum ada peringkat
- Health Economics Research Paper TopicsDokumen5 halamanHealth Economics Research Paper Topicsefj02jba100% (1)
- Nhs Health Check Programme Literature ReviewDokumen6 halamanNhs Health Check Programme Literature Reviewafmzzantalfbfa100% (1)
- Public Health Informatics Review QuestionsDokumen9 halamanPublic Health Informatics Review Questionsapi-326037307100% (1)
- Health Care Policy Research Paper TopicsDokumen4 halamanHealth Care Policy Research Paper Topicsgsrkoxplg100% (1)
- Please Circulate This Document As A Whole or As Individual Questions To Everyone You Can in This Country, and Ask The Recipients To Do The SameDokumen7 halamanPlease Circulate This Document As A Whole or As Individual Questions To Everyone You Can in This Country, and Ask The Recipients To Do The Sameapi-120831962Belum ada peringkat
- Sample Public Health Research PaperDokumen8 halamanSample Public Health Research Paperaflbrozzi100% (1)
- Global Health Dissertation TopicsDokumen5 halamanGlobal Health Dissertation TopicsColumbia100% (1)
- End of Life Care DissertationDokumen8 halamanEnd of Life Care DissertationCustomCollegePapersMadison100% (1)
- Globalisation and Health: Challenges: Go ToDokumen3 halamanGlobalisation and Health: Challenges: Go ToRembrant FernandezBelum ada peringkat
- Innovate, Co-Operate To Improve Health Services For CanadiansLet's Be More Than A Nation of Pilot Projects'by Kimberlyn McGrailDokumen2 halamanInnovate, Co-Operate To Improve Health Services For CanadiansLet's Be More Than A Nation of Pilot Projects'by Kimberlyn McGrailEvidenceNetwork.caBelum ada peringkat
- 5yfv Web PDFDokumen41 halaman5yfv Web PDFjonBelum ada peringkat
- Seeing The Person in The Patient The Point of Care Review Paper Goodrich Cornwell Kings Fund December 2008 0Dokumen76 halamanSeeing The Person in The Patient The Point of Care Review Paper Goodrich Cornwell Kings Fund December 2008 0Levina Benita100% (1)
- Introduction (Story1,2)Dokumen6 halamanIntroduction (Story1,2)3500Belum ada peringkat
- Role of GP in NHSDokumen61 halamanRole of GP in NHSS M Niaz MowlaBelum ada peringkat
- Open Door Case StudyDokumen5 halamanOpen Door Case Studyvinh vũBelum ada peringkat
- Lva1 App6892Dokumen62 halamanLva1 App6892Pallavi PalluBelum ada peringkat
- Healthcare Management Thesis PDFDokumen5 halamanHealthcare Management Thesis PDFmelissabuckleyomaha100% (2)
- Clinician-Scientists in Public Sector Hospitals - Why and HowDokumen3 halamanClinician-Scientists in Public Sector Hospitals - Why and HowPierce ChowBelum ada peringkat
- Director of Public Health Annual Report 2011 12 Section1Dokumen34 halamanDirector of Public Health Annual Report 2011 12 Section1Bijay Kumar MahatoBelum ada peringkat
- An Occupational Health Service in Primary Care: Viewpoint '92Dokumen3 halamanAn Occupational Health Service in Primary Care: Viewpoint '92juan fandiñoBelum ada peringkat
- Thesis Topics in Health InformaticsDokumen5 halamanThesis Topics in Health Informaticsbrendazerrindependence100% (2)
- Attwood & Pedler & Pritchard & Wilkinson (2003) - Leading Change. A Guide To Whole Systems WorkingDokumen225 halamanAttwood & Pedler & Pritchard & Wilkinson (2003) - Leading Change. A Guide To Whole Systems Workingdarky_015Belum ada peringkat
- Health Care Reform Research PapersDokumen8 halamanHealth Care Reform Research Papersmwjhkmrif100% (1)
- Caredata OpenHouse Discussion Points FinalDokumen4 halamanCaredata OpenHouse Discussion Points FinalNHSOpenhouseBelum ada peringkat
- Should NHS Dentistry Be FreeDokumen4 halamanShould NHS Dentistry Be FreePranav SivakumarBelum ada peringkat
- Dissertation Health EconomicsDokumen6 halamanDissertation Health EconomicsBuyCheapPapersOnlineSingapore100% (1)
- First Draft of Business Proposal (Assignment No. 6)Dokumen11 halamanFirst Draft of Business Proposal (Assignment No. 6)Abdullah AmjadBelum ada peringkat
- Unbundling The HospitalDokumen5 halamanUnbundling The Hospitalcrb202Belum ada peringkat
- DR Ross Kerridge Submission To The NSW Inquiry Into Healthcare FundingDokumen5 halamanDR Ross Kerridge Submission To The NSW Inquiry Into Healthcare FundingGabriel FowlerBelum ada peringkat
- Should NHS Dentistry Be FreeDokumen4 halamanShould NHS Dentistry Be FreePranav SivakumarBelum ada peringkat
- 1group B - First DraftDokumen14 halaman1group B - First DraftAbdullah Amjad100% (1)
- Abordaje Clinico 2Dokumen37 halamanAbordaje Clinico 2Samuel Monrroy CervantesBelum ada peringkat
- Uk Public Service Gates FoundatgonDokumen40 halamanUk Public Service Gates Foundatgoneastwind_gBelum ada peringkat
- SJ BDJ 2008Dokumen1 halamanSJ BDJ 2008idurdBelum ada peringkat
- Keogh Review Final ReportDokumen61 halamanKeogh Review Final ReportMennewsdeskBelum ada peringkat
- Public Health Research PapersDokumen7 halamanPublic Health Research Papersp1zajywigyd2100% (1)
- Thesis Statement On HospitalsDokumen5 halamanThesis Statement On Hospitalsbkrj0a1k100% (1)
- Moving Care To The Community: An International PerspectiveDokumen40 halamanMoving Care To The Community: An International PerspectiveWawan Febri RamdaniBelum ada peringkat
- 31 - Can Older Adults Benefitfrom Smart Devices, Wearables, and Other DigitalHealth Options To EnhanceCardiac RehabilitationDokumen9 halaman31 - Can Older Adults Benefitfrom Smart Devices, Wearables, and Other DigitalHealth Options To EnhanceCardiac RehabilitationMariaBelum ada peringkat
- Dian-Consumer Involvement in Health ResearchDokumen12 halamanDian-Consumer Involvement in Health ResearchakfaditadikapariraBelum ada peringkat
- What Passes and Fails As Health Policy and Management: Behind The JargonDokumen14 halamanWhat Passes and Fails As Health Policy and Management: Behind The JargonterenachintyaBelum ada peringkat
- The Slow, Lingering Death of The English NHS: CommentaryDokumen3 halamanThe Slow, Lingering Death of The English NHS: Commentaryzeze_13Belum ada peringkat
- Lithology AbbreviationsDokumen6 halamanLithology AbbreviationsSherif_Abu_You_686Belum ada peringkat
- 3D Seismic Survey Using Swath or Patch-Centered Shooting: A Comparative AnalysisDokumen5 halaman3D Seismic Survey Using Swath or Patch-Centered Shooting: A Comparative Analysiszeze_13Belum ada peringkat
- First Dual-Sensor Ocean Bottom Cable 3D Seismic AcquisitionDokumen13 halamanFirst Dual-Sensor Ocean Bottom Cable 3D Seismic Acquisitionzeze_13Belum ada peringkat
- Energy and Mining Law Newsletter August09Dokumen2 halamanEnergy and Mining Law Newsletter August09zeze_13Belum ada peringkat
- NDEP Annual Report 2014Dokumen91 halamanNDEP Annual Report 2014zeze_13Belum ada peringkat
- PIB Bills Latest 31-5-17.compressedDokumen32 halamanPIB Bills Latest 31-5-17.compressedzeze_13Belum ada peringkat
- Org Culture and Quality ImprovementDokumen17 halamanOrg Culture and Quality Improvementzeze_13Belum ada peringkat
- Openness in OrganisationDokumen10 halamanOpenness in Organisationzeze_13Belum ada peringkat
- OmeprazoleDokumen2 halamanOmeprazoleIvan Matthew SuperioBelum ada peringkat
- CCO Invasive Fungal Disease Downloadable 1Dokumen25 halamanCCO Invasive Fungal Disease Downloadable 1Vasantha KumarBelum ada peringkat
- Sexually Transmitted Diseases in MalesDokumen15 halamanSexually Transmitted Diseases in MalesSam Raven AndresBelum ada peringkat
- Service Quality Patient Satisfaction and Loyalty in The Bangladesh Healthcare SectorDokumen14 halamanService Quality Patient Satisfaction and Loyalty in The Bangladesh Healthcare Sectorgubbare86Belum ada peringkat
- Factors Affecting Sleep: The Quality and Quantity of Sleep AreDokumen3 halamanFactors Affecting Sleep: The Quality and Quantity of Sleep AreBijali sinha100% (3)
- A Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesDokumen6 halamanA Novel Clinical Grading Scale To Guide The Management of Crusted ScabiesFelisiana KasmanBelum ada peringkat
- Soal PAS BIG Xi, SMT 3, OnlineDokumen10 halamanSoal PAS BIG Xi, SMT 3, OnlineRivaldi Lukman HakimBelum ada peringkat
- The Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanDokumen5 halamanThe Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanshubhangivsBelum ada peringkat
- Contoh FMEA UIHC Burn Unit Patient Education DocumentationDokumen2 halamanContoh FMEA UIHC Burn Unit Patient Education DocumentationAnisaBelum ada peringkat
- NeuropsychiatryDokumen5 halamanNeuropsychiatryNicole TangcoBelum ada peringkat
- School Feeding Standards and School-Based Program Implementation ReviewDokumen60 halamanSchool Feeding Standards and School-Based Program Implementation ReviewGem Lam SenBelum ada peringkat
- Aggregates - Limestone Dolomite Safety Data SheetDokumen8 halamanAggregates - Limestone Dolomite Safety Data SheetJEAN KATHLEEN SORIANOBelum ada peringkat
- Treatment and Prevention of LeptospirosisDokumen7 halamanTreatment and Prevention of LeptospirosisSherry FeliciaBelum ada peringkat
- Food Science and Nutrition (FSN) - Cal Poly Catalog - FSNDokumen6 halamanFood Science and Nutrition (FSN) - Cal Poly Catalog - FSNmyelkenBelum ada peringkat
- SMR August 19 (Rengat - Tembilahan, Sect 2) PDFDokumen28 halamanSMR August 19 (Rengat - Tembilahan, Sect 2) PDFDoo PLTGUBelum ada peringkat
- MCN Lec M1L1 ReviewerDokumen4 halamanMCN Lec M1L1 ReviewerEmily BernatBelum ada peringkat
- Recommendations For Cardiovascular Prevention DuringDokumen5 halamanRecommendations For Cardiovascular Prevention DuringRaiyanBelum ada peringkat
- Effects of Healthcare EnvironmentsDokumen11 halamanEffects of Healthcare EnvironmentsJoanna AngelopoulouBelum ada peringkat
- Segurança e Tax de Lesoes PDFDokumen20 halamanSegurança e Tax de Lesoes PDFFilipeAssunçãoBelum ada peringkat
- Vilas County News-Review, March 14, 2012 - SECTION BDokumen10 halamanVilas County News-Review, March 14, 2012 - SECTION BNews-ReviewBelum ada peringkat