Anda mungkin juga menyukai
- Impacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandImpacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Fractured Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandFractured Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Non-Caries Dental DiseaseDokumen61 halamanNon-Caries Dental Diseaseapi-19916399Belum ada peringkat
- Aa 1 MasterRQsDokumen93 halamanAa 1 MasterRQsSadhana SabhandasaniBelum ada peringkat
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDokumen39 halamanAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyBelum ada peringkat
- Orthodonticsdd2011-2012 DR GhadeerDokumen62 halamanOrthodonticsdd2011-2012 DR GhadeerGhadeerHassaan100% (1)
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Dokumen15 halamanA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- (DD13-14) Dental AnatomyDokumen443 halaman(DD13-14) Dental AnatomyJacobsen RichardBelum ada peringkat
- Periodontal Diseases in Children PedoDokumen34 halamanPeriodontal Diseases in Children PedoFourthMolar.comBelum ada peringkat
- 300 DA Facts For NBDE IDokumen13 halaman300 DA Facts For NBDE IAarrthi SBelum ada peringkat
- Endodontics PDFDokumen109 halamanEndodontics PDFduracell19Belum ada peringkat
- INBDE Test Specifications, by Clinical Component Section: Diagnosis and Treatment Planning Practice and ProfessionDokumen3 halamanINBDE Test Specifications, by Clinical Component Section: Diagnosis and Treatment Planning Practice and ProfessionHanin AbukhiaraBelum ada peringkat
- Pulp Therapy For Primary and Immature Permanent TeethDokumen11 halamanPulp Therapy For Primary and Immature Permanent TeethPrabhjot KaurBelum ada peringkat
- Causes of Endodontic FailuresDokumen8 halamanCauses of Endodontic Failuresizeldien5870Belum ada peringkat
- Clinical Portfolio EndoDokumen16 halamanClinical Portfolio EndodrhijaziBelum ada peringkat
- Nbde01 Examinee GuideDokumen36 halamanNbde01 Examinee GuideHKBelum ada peringkat
- Ndodontic Iagnosis: by Clifford J. Ruddle, D.D.SDokumen10 halamanNdodontic Iagnosis: by Clifford J. Ruddle, D.D.Srojek63Belum ada peringkat
- 03 MFDS Regulations & Syllabus 2011Dokumen15 halaman03 MFDS Regulations & Syllabus 2011FarahMohammed1Belum ada peringkat
- Systemic Diseases Manifested in The JawsDokumen25 halamanSystemic Diseases Manifested in The JawsTeguh Caninus100% (1)
- Pickard's Manual-Tooth Wear (Dragged)Dokumen8 halamanPickard's Manual-Tooth Wear (Dragged)Adit MehtaBelum ada peringkat
- Immediate Dentures - 2Dokumen18 halamanImmediate Dentures - 2Ayad IbrahimBelum ada peringkat
- Aetiology of Malocclusion of The TeethDokumen2 halamanAetiology of Malocclusion of The TeethBob Permana Simanungkalit100% (1)
- Department of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearDokumen29 halamanDepartment of Pedodontics: Submitted By: Shayoni Sen Bds Ivth YearFarzana ShereenBelum ada peringkat
- 11 Glass - Ionomer MaterialsDokumen36 halaman11 Glass - Ionomer MaterialsPepo BelovedBelum ada peringkat
- Comments Nbde ExamsDokumen9 halamanComments Nbde ExamsMark GebrailBelum ada peringkat
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDokumen6 halamanEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargBelum ada peringkat
- Periodontal Therapy StatementDokumen7 halamanPeriodontal Therapy StatementDiana AlexandraBelum ada peringkat
- Good Morning.: @areebazainabDokumen42 halamanGood Morning.: @areebazainabshabana waniBelum ada peringkat
- Endodontic Management of Traumatic InjuriesDokumen6 halamanEndodontic Management of Traumatic InjuriesMehwish MunawarBelum ada peringkat
- Omsb Orthodontic Prometric Text Content and Test ReferencesDokumen1 halamanOmsb Orthodontic Prometric Text Content and Test ReferencesAli AlyaBelum ada peringkat
- Mounting Dental X-RaysDokumen6 halamanMounting Dental X-RaysZahid AhmadBelum ada peringkat
- Management of Odontogenic Infections and SepsisDokumen8 halamanManagement of Odontogenic Infections and Sepsismartha carolina vargas bernalBelum ada peringkat
- NBDE NotesDokumen2 halamanNBDE NotesAbhay KhannaBelum ada peringkat
- Guidelines BookDokumen16 halamanGuidelines BookAdel ElaroudBelum ada peringkat
- Etiology of Periodontal Diseases - II - Role of Calculus and Local FactorsDokumen33 halamanEtiology of Periodontal Diseases - II - Role of Calculus and Local FactorsHeba S RadaidehBelum ada peringkat
- Peridontal Pocket PerioDokumen29 halamanPeridontal Pocket PerioFourthMolar.comBelum ada peringkat
- 1Dokumen49 halaman1Asma'a AlmawasBelum ada peringkat
- Periodon TicsDokumen201 halamanPeriodon TicsmirfanulhaqBelum ada peringkat
- Written Examination GuideDokumen17 halamanWritten Examination GuideIhsan HanbaliBelum ada peringkat
- Oral Path I CombinedDokumen68 halamanOral Path I CombinedkmcalleBelum ada peringkat
- Tooth DevelopmentDokumen36 halamanTooth DevelopmentDaffa YudhistiraBelum ada peringkat
- Pulp and Periapical: - Also Notes From Biopsy TechniquesDokumen31 halamanPulp and Periapical: - Also Notes From Biopsy TechniquesmythaiuBelum ada peringkat
- Periodontal Problems in KidsDokumen49 halamanPeriodontal Problems in KidsRaksmey PhanBelum ada peringkat
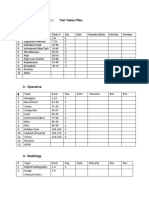
- NBDE PART 2::::::::::::::::::: Test Takers Plan 1. EndodonticsDokumen6 halamanNBDE PART 2::::::::::::::::::: Test Takers Plan 1. EndodonticsDr yones SobhyBelum ada peringkat
- Articaine Dental Update 2015Dokumen5 halamanArticaine Dental Update 2015Ashley WrightBelum ada peringkat
- (DD13 14) Bio PhysioDokumen587 halaman(DD13 14) Bio PhysiominiarBelum ada peringkat
- Oral PathDokumen49 halamanOral PathAnca NeaguBelum ada peringkat
- Wiley - Clinical Cases in Orthodontics - 978-1-118-29247-1Dokumen2 halamanWiley - Clinical Cases in Orthodontics - 978-1-118-29247-1MayerBelum ada peringkat
- Foreign Trained Dentists To US - FullDokumen8 halamanForeign Trained Dentists To US - Fullh20pologt100% (1)
- Extrac 1Dokumen49 halamanExtrac 1api-19916399Belum ada peringkat
- Dentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableDokumen22 halamanDentosphere - World of Dentistry - MCQs On Skin and Vesiculobullous Diseases - Or-SearchableAssssssBelum ada peringkat
- PeriodonticsDokumen162 halamanPeriodonticsdr_rushik100% (1)
- Technological Advances in Nontraditional Orthodontics PDFDokumen14 halamanTechnological Advances in Nontraditional Orthodontics PDFcatherineBelum ada peringkat
- Sample Questions MJDF Part 1 Sample Questions MJDF Part 1Dokumen21 halamanSample Questions MJDF Part 1 Sample Questions MJDF Part 1HarkanBelum ada peringkat
- Very Imp DocsDokumen43 halamanVery Imp DocsKareem ShawaBelum ada peringkat
- Prometric 2Dokumen4 halamanPrometric 2zoaib aliBelum ada peringkat
- Syllabus 5k en ExamDokumen2 halamanSyllabus 5k en ExamVagelis RaftopoulosBelum ada peringkat
- Essential Tissue Healing of the Face and NeckDari EverandEssential Tissue Healing of the Face and NeckPenilaian: 5 dari 5 bintang5/5 (2)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDari EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideBelum ada peringkat
- White Spot Lesion Formation Prevention TreatmentDokumen9 halamanWhite Spot Lesion Formation Prevention TreatmentRubén Godoy CisternasBelum ada peringkat
- Ijerph2007010008 PDFDokumen8 halamanIjerph2007010008 PDFtjangkanBelum ada peringkat
- Comparative Assessment of Pak National Drinking Water Quality StandardsDokumen15 halamanComparative Assessment of Pak National Drinking Water Quality StandardsMujjo SahbBelum ada peringkat
- Diseases of Hard Tissues of Teeth PDFDokumen152 halamanDiseases of Hard Tissues of Teeth PDFAPARNA AARATHI SREEKUMARBelum ada peringkat
- Removal of Fluoride From Water by Five Submerged PlantsDokumen5 halamanRemoval of Fluoride From Water by Five Submerged PlantsdyahprastiwiaBelum ada peringkat
- Snoring Smile Green DentistryDokumen24 halamanSnoring Smile Green DentistryNaseer JahanBelum ada peringkat
- White SpotsDokumen24 halamanWhite SpotsDonanguyenBelum ada peringkat
- Measuring Dental DiseasesDokumen19 halamanMeasuring Dental DiseasesmisdduaaBelum ada peringkat
- Bleaching Part 1Dokumen6 halamanBleaching Part 1Hamad KayaniBelum ada peringkat
- Abstract Book-DraftDokumen60 halamanAbstract Book-DraftMTehseenRajputBelum ada peringkat
- Fluoride Toxicity and DefluoridationDokumen91 halamanFluoride Toxicity and DefluoridationAbhijeet Kadu50% (2)
- Fluoride Contamination in Groundwater in Some Villages of Banda District, Uttar Pradesh, IndiaDokumen4 halamanFluoride Contamination in Groundwater in Some Villages of Banda District, Uttar Pradesh, IndiaIJIRSTBelum ada peringkat
- The Concentration of Fluorides in Tap Water and Commercial Bottled Beverages in Cazma-Northen CroatiaDokumen18 halamanThe Concentration of Fluorides in Tap Water and Commercial Bottled Beverages in Cazma-Northen CroatiaSilvana KrmekBelum ada peringkat
- ANNUAL REPORT 2011-12: The Rotary Foundation Rotary InternationalDokumen40 halamanANNUAL REPORT 2011-12: The Rotary Foundation Rotary InternationalRjendra LamsalBelum ada peringkat
- Fluoridation - Seminar TopicDokumen4 halamanFluoridation - Seminar Topicnawafaslam100% (1)
- Micro and MacroDokumen28 halamanMicro and MacroMadhana MadhubalaBelum ada peringkat
- Effective Interventions To Prevent Dental Caries in Preschool ChildrenDokumen56 halamanEffective Interventions To Prevent Dental Caries in Preschool ChildrenDiego AzaedoBelum ada peringkat
- The Duperstate: " - An Epic 12 Page Internet Novel in 1 MB PDF Format A True Story About Selling You HardcoreDokumen26 halamanThe Duperstate: " - An Epic 12 Page Internet Novel in 1 MB PDF Format A True Story About Selling You HardcorePaul Reverelike100% (4)
- History of FluoridationDokumen49 halamanHistory of FluoridationTin MawBelum ada peringkat
- Fluoride in Drinking - Water - Status - Issues - and - SolutionsDokumen208 halamanFluoride in Drinking - Water - Status - Issues - and - SolutionsAlto CodeBelum ada peringkat
- Infiltration, A New Therapy For Masking Enamel White Spot PDFDokumen12 halamanInfiltration, A New Therapy For Masking Enamel White Spot PDFwijayanti siswantoBelum ada peringkat
- Fluoride: Quarterly Journal of The International Society For Fluoride Research IncDokumen6 halamanFluoride: Quarterly Journal of The International Society For Fluoride Research IncNain NoorBelum ada peringkat
- PSM Prep LadderDokumen43 halamanPSM Prep LadderMayanka SaxenaBelum ada peringkat
- 2012 BHAA ProceedingsDokumen348 halaman2012 BHAA ProceedingsBHAAChicagoBelum ada peringkat
- Nutritional Problems in IndiaDokumen87 halamanNutritional Problems in IndiaMubarak Meera Sahib80% (25)
- Tooth Brushing Behaviors and Fluoridated Toothpaste Use Among Children Younger Than Three Years Old in ChicagoDokumen8 halamanTooth Brushing Behaviors and Fluoridated Toothpaste Use Among Children Younger Than Three Years Old in ChicagoFaiqotul KumalaBelum ada peringkat
- NFS 382 Final ReviewDokumen56 halamanNFS 382 Final ReviewAya ThairBelum ada peringkat
- CH 18 PDFDokumen19 halamanCH 18 PDFkrishnaBelum ada peringkat
- March 2 Pages - Gowrie NewsDokumen12 halamanMarch 2 Pages - Gowrie NewsTonya HarrisonBelum ada peringkat
- Guidelines On The Use of Fuoride For Caries Prevention in Children An Updated EAPD Policy DocumentDokumen10 halamanGuidelines On The Use of Fuoride For Caries Prevention in Children An Updated EAPD Policy DocumentIrene ChuangBelum ada peringkat