Anda mungkin juga menyukai
- CFCSDokumen77 halamanCFCSNurul NadiahBelum ada peringkat
- Knowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health ClinicDokumen7 halamanKnowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health Clinic2A - Nicole Marrie Honrado100% (1)
- 02.borang Diabetes Clinical Audit MELAYUDokumen3 halaman02.borang Diabetes Clinical Audit MELAYUnorhaslizaBelum ada peringkat
- Oscc CmeDokumen97 halamanOscc CmeKernYen LeeBelum ada peringkat
- RCPI Management of Early Pregnancy MiscarriageDokumen24 halamanRCPI Management of Early Pregnancy MiscarriagerazorazBelum ada peringkat
- Explanation LetterDokumen1 halamanExplanation LettersaufisafingiBelum ada peringkat
- Log Book GCFM MockDokumen135 halamanLog Book GCFM Mocknurul asyikin abdullahBelum ada peringkat
- PartogramDokumen9 halamanPartogramrosdi_ponBelum ada peringkat
- ATUCU5 - 20191018 - FA Edit 11.11.2020 - Compressed PDFDokumen172 halamanATUCU5 - 20191018 - FA Edit 11.11.2020 - Compressed PDFSheral AidaBelum ada peringkat
- Febrile Seizures Epilepsy OSCE Counselling PaediatricsDokumen6 halamanFebrile Seizures Epilepsy OSCE Counselling PaediatricsJJ Lim100% (1)
- Anti-Gout AgentDokumen42 halamanAnti-Gout AgentSaha DirllahBelum ada peringkat
- Edward SyndromeDokumen11 halamanEdward SyndromeVikneswaran VîçkýBelum ada peringkat
- Clerking An o & G CaseDokumen57 halamanClerking An o & G CaseAlan Na100% (2)
- Dysmenorrhea: LINDA FRENCH, M.D., Michigan State University College of Human Medicine, East Lansing, MichiganDokumen7 halamanDysmenorrhea: LINDA FRENCH, M.D., Michigan State University College of Human Medicine, East Lansing, MichiganJosieBelum ada peringkat
- GDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsDokumen3 halamanGDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsBabarNaeemBelum ada peringkat
- Management of OSCC CaseDokumen40 halamanManagement of OSCC CaseMagdalene Choo Yenli100% (1)
- Clerking Guide Obstetrics CasesDokumen3 halamanClerking Guide Obstetrics CasesNorFarah Fatin AnuarBelum ada peringkat
- Merci NoteDokumen2 halamanMerci NoteSubbash EkambaramBelum ada peringkat
- OADokumen27 halamanOADarkKnighthere100% (1)
- Physical Examination of Orthopedic Patients: Dr. M. Bayu, Sp. OTDokumen55 halamanPhysical Examination of Orthopedic Patients: Dr. M. Bayu, Sp. OTsurya gunawanBelum ada peringkat
- Assisted Reproductive Technology: Project ReportDokumen9 halamanAssisted Reproductive Technology: Project ReportanaghaBelum ada peringkat
- CWU OrthopedicsDokumen6 halamanCWU OrthopedicsSana Anam JahanBelum ada peringkat
- Assisted Reproductive TechniquesDokumen146 halamanAssisted Reproductive TechniquesGouravBelum ada peringkat
- Patient History Questionnaire: Last FirstDokumen5 halamanPatient History Questionnaire: Last FirstMizuiro SenpaiBelum ada peringkat
- SPUP School of Medicine: Smyle/MABCDokumen9 halamanSPUP School of Medicine: Smyle/MABCJOnapz Santos UnisTaBelum ada peringkat
- Patient History QuestionnaireDokumen6 halamanPatient History QuestionnaireAries BautistaBelum ada peringkat
- Cburbachcareplan 2Dokumen8 halamanCburbachcareplan 2api-520843051Belum ada peringkat
- TonsillitisDokumen5 halamanTonsillitisyosefBelum ada peringkat
- Patient History ObgynDokumen4 halamanPatient History ObgynThree ZeroBelum ada peringkat
- Uti Case PresentationDokumen29 halamanUti Case Presentationsalma.nasr003100% (1)
- Urinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorDokumen11 halamanUrinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorJim Jose AntonyBelum ada peringkat
- Obgyn PT HistoryDokumen4 halamanObgyn PT HistoryDr. SheikhBelum ada peringkat
- SOAP Note - ContraceptionDokumen5 halamanSOAP Note - ContraceptionG. Crusor-PriceBelum ada peringkat
- A. HestiantoroThe Journey of Endometriosis Patients in Indonesia Seek Care Indonesian ExperienceDokumen19 halamanA. HestiantoroThe Journey of Endometriosis Patients in Indonesia Seek Care Indonesian ExperienceAnnisa YutamiBelum ada peringkat
- Client Care Study On Typhoid FeverDokumen31 halamanClient Care Study On Typhoid Fevernsrafel0Belum ada peringkat
- Nursing Care 2Dokumen1 halamanNursing Care 2Moh. H.AlObaidyBelum ada peringkat
- Pregnancy Follow UpDokumen17 halamanPregnancy Follow UpE. Zeynep YilmazBelum ada peringkat
- Management of Sexually Transmitted Diseases and Hiv AidsDokumen28 halamanManagement of Sexually Transmitted Diseases and Hiv AidsUtkarsh YadavBelum ada peringkat
- Womens Health - Soap Note 1Dokumen11 halamanWomens Health - Soap Note 1api-494643478100% (2)
- Necrotising Enterocolitis in Infants On NICU JCG0038 v2Dokumen11 halamanNecrotising Enterocolitis in Infants On NICU JCG0038 v2RatnaArdianaNoviantiBelum ada peringkat
- Case Study TBDokumen8 halamanCase Study TBCesar Emmanuel Abigania100% (2)
- Gyn Revalida Review CSL 2 2017Dokumen101 halamanGyn Revalida Review CSL 2 2017Mara Medina - BorleoBelum ada peringkat
- Sti Management and PitfallsDokumen39 halamanSti Management and PitfallsDr.Lakshmiprasad LBelum ada peringkat
- IBD Surgical AlgorithmDokumen30 halamanIBD Surgical AlgorithmKarthik SubramaniamBelum ada peringkat
- Urinary Tract Infections in ChildrenDokumen16 halamanUrinary Tract Infections in ChildrenPraluki HerliawanBelum ada peringkat
- Maternal NSG ProceduresDokumen18 halamanMaternal NSG ProceduresGARCIA, KYLA MAE A.Belum ada peringkat
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Dokumen6 halamanPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieBelum ada peringkat
- MANILA HEALTH DEAPRTMENT ProfileDokumen21 halamanMANILA HEALTH DEAPRTMENT ProfileJen Ballesteros100% (7)
- Viva 1 Family Medicine Group E: ImmunisationDokumen5 halamanViva 1 Family Medicine Group E: ImmunisationZambriBelum ada peringkat
- Pelvic Inflammatory Disease (PID)Dokumen16 halamanPelvic Inflammatory Disease (PID)CHRISTIAN RAY ALPAS PASILIAOBelum ada peringkat
- Overview of Sti'S: DR - Aruna Kumari.D. MBBS, DVD, MHA QPCC&C, Ministry of HealthDokumen56 halamanOverview of Sti'S: DR - Aruna Kumari.D. MBBS, DVD, MHA QPCC&C, Ministry of HealthDCBBelum ada peringkat
- Family Medicine HU Past PapersDokumen141 halamanFamily Medicine HU Past Papersأجمل أصوات الشيوخBelum ada peringkat
- Congenital SyphilisDokumen1 halamanCongenital SyphilisAparna Devi100% (1)
- Presentasi Pengobatan TB RO Pada AnakDokumen93 halamanPresentasi Pengobatan TB RO Pada Anakdr_eko_pBelum ada peringkat
- Infections in OB/GYN: Vaginitis, STI'sDokumen52 halamanInfections in OB/GYN: Vaginitis, STI'sMiftahurrahmah GmsBelum ada peringkat
- Genital HerpesDokumen4 halamanGenital Herpesmarie andreBelum ada peringkat
- NCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & AidsDokumen20 halamanNCM 112: Nursing Care of Sexually-Transmitted Infections, Hiv Infections & Aidsfebie pachecoBelum ada peringkat
- 13lec Dealing With HIV and Other STIs in The AdolescentsDokumen39 halaman13lec Dealing With HIV and Other STIs in The AdolescentsGilihac EgrojBelum ada peringkat
- Vaginal Infections Update: Original ReviewDokumen6 halamanVaginal Infections Update: Original ReviewEpi PanjaitanBelum ada peringkat
- History, Physical Examination and Preventive Health Care: Jeezreel M. Orquina, RN, LPTDokumen30 halamanHistory, Physical Examination and Preventive Health Care: Jeezreel M. Orquina, RN, LPTLaiza MontonBelum ada peringkat
- Child Abuse and Neglect DR NorazlinDokumen59 halamanChild Abuse and Neglect DR NorazlinSuhazeli AbdullahBelum ada peringkat
- Immunocompromise State in Pregnancy 2013Dokumen51 halamanImmunocompromise State in Pregnancy 2013Suhazeli Abdullah100% (1)
- Dr. Nik Rubiah 040713 (Latest)Dokumen28 halamanDr. Nik Rubiah 040713 (Latest)Suhazeli Abdullah100% (1)
- SOSCG 6jul2013 v5Dokumen32 halamanSOSCG 6jul2013 v5Suhazeli Abdullah100% (2)
- TB CPG DR Jamalul AzizDokumen71 halamanTB CPG DR Jamalul AzizSuhazeli AbdullahBelum ada peringkat
- Measles FM S 05072013Dokumen42 halamanMeasles FM S 05072013Suhazeli AbdullahBelum ada peringkat
- Plasmodium Knowlesi Infection - A New ThreatDokumen31 halamanPlasmodium Knowlesi Infection - A New ThreatSuhazeli AbdullahBelum ada peringkat
- Role of Larc For Unmet Needs in ContraceptionDokumen37 halamanRole of Larc For Unmet Needs in ContraceptionSuhazeli AbdullahBelum ada peringkat
- Clinical Research MalaysiaDokumen16 halamanClinical Research MalaysiaSuhazeli AbdullahBelum ada peringkat
- How To PublishDokumen24 halamanHow To PublishSuhazeli AbdullahBelum ada peringkat
- CerazetteDokumen36 halamanCerazetteSuhazeli AbdullahBelum ada peringkat
- IMCI Plan C 2013Dokumen51 halamanIMCI Plan C 2013Suhazeli AbdullahBelum ada peringkat
- Chart Booklet National Mac 2012Dokumen42 halamanChart Booklet National Mac 2012Suhazeli AbdullahBelum ada peringkat
- Microbiology and Parasitology1Dokumen249 halamanMicrobiology and Parasitology1Keshi Wo100% (3)
- Lab 7 Genus NeisseriaDokumen20 halamanLab 7 Genus NeisseriaAAABelum ada peringkat
- Neisseria, MoraxellaDokumen33 halamanNeisseria, MoraxellaShuler0071Belum ada peringkat
- 2006-02-16Dokumen12 halaman2006-02-16The University Daily KansanBelum ada peringkat
- Psychology Internals ContentDokumen23 halamanPsychology Internals ContentMohit KapseBelum ada peringkat
- Yousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Dokumen147 halamanYousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Amr AmalBelum ada peringkat
- Vulvovaginitis (POGS 2009)Dokumen13 halamanVulvovaginitis (POGS 2009)JEREMIE FAYE UMALIBelum ada peringkat
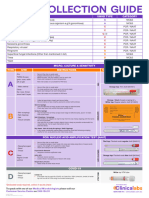
- Swab GuideDokumen1 halamanSwab GuideKarim SirBelum ada peringkat
- Textbook of Diagnostic Microbiology 4th Edition Mahon Test BankDokumen13 halamanTextbook of Diagnostic Microbiology 4th Edition Mahon Test Banklaylafarleyh3i8j9100% (26)
- Sexually Transmitted Diseases (STDS) : Unit OneDokumen12 halamanSexually Transmitted Diseases (STDS) : Unit OneBol Manyuol AyuelBelum ada peringkat
- Step2 CS NotesDokumen50 halamanStep2 CS Notesvarrakesh100% (1)
- Best Insight Specialty-Paeds TeamDokumen56 halamanBest Insight Specialty-Paeds TeamSaQlain BalochBelum ada peringkat
- STD 101Dokumen42 halamanSTD 101Clarice BedicoBelum ada peringkat
- Newborns Undergo Profound Physiologic Changes at The Moment of BirthDokumen8 halamanNewborns Undergo Profound Physiologic Changes at The Moment of BirthUri ELBelum ada peringkat
- Bacterial Urinary Tract InfectionDokumen17 halamanBacterial Urinary Tract InfectionROSANNA BUCAGBelum ada peringkat
- 10th Lecture (NCM 104 CD II) Care of Clients With Problems inDokumen23 halaman10th Lecture (NCM 104 CD II) Care of Clients With Problems inIcka Fong50% (4)
- REVIEW QUESTIONS For MIDTERMSDokumen107 halamanREVIEW QUESTIONS For MIDTERMSReign FloresBelum ada peringkat
- Name Address City State Zipcode Toll Free Website DescriptionDokumen21 halamanName Address City State Zipcode Toll Free Website Descriptionapi-18351628Belum ada peringkat
- CDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesDokumen7 halamanCDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesAhmad Arbi AninditoBelum ada peringkat
- Clin Pharm - Handbook Pharmacotherapy 9thDokumen10 halamanClin Pharm - Handbook Pharmacotherapy 9thstella.gillesania.chenBelum ada peringkat
- Risk Factors of Gonorhea Infection Among Indirect Female Sex Workers (Ifsw) in Indonesia 2015 ArticleDokumen6 halamanRisk Factors of Gonorhea Infection Among Indirect Female Sex Workers (Ifsw) in Indonesia 2015 ArticleFrans LandiBelum ada peringkat
- Sexually Transmitted DiseasesDokumen76 halamanSexually Transmitted Diseasessomaya abdulhakimBelum ada peringkat
- The History of Venereal Disease and Parangi in Sri LankaDokumen6 halamanThe History of Venereal Disease and Parangi in Sri LankaMindStilledBelum ada peringkat
- 10.0 Reproductive SystemDokumen64 halaman10.0 Reproductive SystemMichelle GalvanBelum ada peringkat
- GuidelinesforSTISurveillance1999 EnglishDokumen46 halamanGuidelinesforSTISurveillance1999 EnglishjoreyvilBelum ada peringkat
- Health Related Fitness TestDokumen6 halamanHealth Related Fitness TestAimee HernandezBelum ada peringkat
- Health 8 - 4th Quarter LessonsDokumen7 halamanHealth 8 - 4th Quarter LessonsaeonniobeBelum ada peringkat
- IRaMuTeQ Tutorial Translated To English - 17.03.2016Dokumen35 halamanIRaMuTeQ Tutorial Translated To English - 17.03.2016subasamjadBelum ada peringkat
- b3 Infection and Response Mastery Booklet v3Dokumen20 halamanb3 Infection and Response Mastery Booklet v3laurnawhittakerBelum ada peringkat
- Common Sexually Transmitted Diseases: STD 101 For CliniciansDokumen68 halamanCommon Sexually Transmitted Diseases: STD 101 For CliniciansAnonymous h2EnKyDbBelum ada peringkat