Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The China Study PDFDokumen7 halamanThe China Study PDFPatrice108365Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Brigham Intensive Review of Internal Medicine Q&A Companion, 2eDokumen227 halamanThe Brigham Intensive Review of Internal Medicine Q&A Companion, 2eMalueth Angui100% (4)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Eric Berg CVDokumen6 halamanEric Berg CVHaralambicBelum ada peringkat
- Interpretting ABG SuccessfullyDokumen15 halamanInterpretting ABG Successfullyanimathz100% (1)
- What is BronchoscopyDokumen19 halamanWhat is BronchoscopyMARIANN JEAN ANDREA CULANAG MATALINESBelum ada peringkat
- B. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseDokumen4 halamanB. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseSOLEIL LOUISE LACSON MARBAS100% (1)
- Extra Oral RadiographyDokumen17 halamanExtra Oral RadiographyAl RawdhaBelum ada peringkat
- Contrast Media UsedDokumen3 halamanContrast Media UsedAl RawdhaBelum ada peringkat
- Antibiotics Part 1Dokumen32 halamanAntibiotics Part 1Al RawdhaBelum ada peringkat
- Dental health in pregnancy guideDokumen18 halamanDental health in pregnancy guideAl RawdhaBelum ada peringkat
- Easy NotesDokumen8 halamanEasy NotesAl RawdhaBelum ada peringkat
- Elimination of A DrugDokumen8 halamanElimination of A DrugAl RawdhaBelum ada peringkat
- Applied Physiology of Cardio Vascular SystemDokumen15 halamanApplied Physiology of Cardio Vascular SystemAl RawdhaBelum ada peringkat
- Anatomy of Trigeminal Nerve - FinalDokumen14 halamanAnatomy of Trigeminal Nerve - FinalAl RawdhaBelum ada peringkat
- Drug Safety ListDokumen2 halamanDrug Safety ListTri Hapsoro GunoBelum ada peringkat
- Sailography PorcedureDokumen2 halamanSailography PorcedureAl RawdhaBelum ada peringkat
- Old Questions 1Dokumen23 halamanOld Questions 1Al RawdhaBelum ada peringkat
- Statistical Selection GuideDokumen2 halamanStatistical Selection GuideRajanedi Rama KrishnaBelum ada peringkat
- Advancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewDokumen5 halamanAdvancement in Diagnostic Aids For Oral Premalignant Lesions: A ReviewAl RawdhaBelum ada peringkat
- Preliminary Communications: HyperosmolarDokumen3 halamanPreliminary Communications: HyperosmolarAl RawdhaBelum ada peringkat
- Antifungal Activity of Xylitol Against ICandida Albicansi An Iin Vitroi StudyDokumen5 halamanAntifungal Activity of Xylitol Against ICandida Albicansi An Iin Vitroi StudyAl RawdhaBelum ada peringkat
- Anil NandaDokumen5 halamanAnil NandaAl RawdhaBelum ada peringkat
- Genetic Etiologies of Facial CleftingDokumen15 halamanGenetic Etiologies of Facial CleftingAl RawdhaBelum ada peringkat
- PRISMA 2009 Checklist: An AnalysisDokumen2 halamanPRISMA 2009 Checklist: An AnalysisFiŗåš ÀßßâşBelum ada peringkat
- Recent Advances in Dental Sciences: Nevus of Ota: A Rare Case With Review of LiteratureDokumen4 halamanRecent Advances in Dental Sciences: Nevus of Ota: A Rare Case With Review of LiteratureAl RawdhaBelum ada peringkat
- 1 s2.0 S2212440316300104 MainDokumen11 halaman1 s2.0 S2212440316300104 MainAl RawdhaBelum ada peringkat
- 1 s2.0 S2212440316300104 MainDokumen11 halaman1 s2.0 S2212440316300104 MainAl RawdhaBelum ada peringkat
- CHARTINGDokumen17 halamanCHARTINGAl RawdhaBelum ada peringkat
- CBCT How Does It Work Scarfe Et Al 2008 (4pdf)Dokumen24 halamanCBCT How Does It Work Scarfe Et Al 2008 (4pdf)KannaBelum ada peringkat
- Resistance Index in Mediastinal Lymph Nodes: A Feasibility StudyDokumen3 halamanResistance Index in Mediastinal Lymph Nodes: A Feasibility StudyAl RawdhaBelum ada peringkat
- Recognisation of Proteins Sp. To OKC FluidsDokumen8 halamanRecognisation of Proteins Sp. To OKC FluidsAl RawdhaBelum ada peringkat
- Classification and TerminologyDokumen8 halamanClassification and TerminologyAl RawdhaBelum ada peringkat
- Recent Advances in Immunofluorescent Tests and Its Applications in Oral DiagnosisDokumen3 halamanRecent Advances in Immunofluorescent Tests and Its Applications in Oral DiagnosisAl RawdhaBelum ada peringkat
- RadiologyDokumen9 halamanRadiologyAl RawdhaBelum ada peringkat
- Review of OSMFDokumen10 halamanReview of OSMFAl RawdhaBelum ada peringkat
- National Institute of Occupational Safety and Health Course CurriculumDokumen9 halamanNational Institute of Occupational Safety and Health Course Curriculummohan dassBelum ada peringkat
- Askep CKD Bhs InggrisDokumen15 halamanAskep CKD Bhs InggrisFitri MulyaBelum ada peringkat
- Prevalence of Hypothyroidism in Adults An EpidemioDokumen6 halamanPrevalence of Hypothyroidism in Adults An EpidemioCindy Auliah NasutionBelum ada peringkat
- Sgot & SGPTDokumen2 halamanSgot & SGPT우영박Belum ada peringkat
- Position Paper On Teenage PregnancyDokumen3 halamanPosition Paper On Teenage PregnancyMark Anthony CabangonBelum ada peringkat
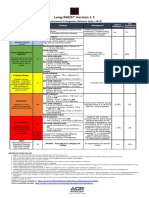
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- Triage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDDokumen6 halamanTriage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDRatna SariBelum ada peringkat
- RNA Non Enveloped VirusesDokumen35 halamanRNA Non Enveloped VirusesRPh Krishna Chandra JagritBelum ada peringkat
- Ann JeinaDokumen7 halamanAnn JeinaMizumoriFumairaBelum ada peringkat
- Myocardial InfarctionDokumen18 halamanMyocardial InfarctionMarc Lorenz DucusinBelum ada peringkat
- ImmunosuppresentsDokumen13 halamanImmunosuppresentsmadeputraBelum ada peringkat
- Aula 1Dokumen14 halamanAula 1Brigida Cirqueira GuimaraesBelum ada peringkat
- Oral Pathology Hereditary Conditions: Group IDokumen74 halamanOral Pathology Hereditary Conditions: Group IFatima CarlosBelum ada peringkat
- Full Body To Body Massage Centre in MG Road Gurgaon Delhi NCRDokumen11 halamanFull Body To Body Massage Centre in MG Road Gurgaon Delhi NCRFlip Body SpaBelum ada peringkat
- 5a.ESOPHAGEAL DISORDERSDokumen16 halaman5a.ESOPHAGEAL DISORDERSHayat AL AKOUMBelum ada peringkat
- Global Tuberculosis Report 2018 PDFDokumen243 halamanGlobal Tuberculosis Report 2018 PDFDudungBelum ada peringkat
- Type2 Diabetes HandoutDokumen1 halamanType2 Diabetes Handouthendra_darmawan_4Belum ada peringkat
- Complications of 3rd TrimesterDokumen49 halamanComplications of 3rd TrimesterMA. JYRELL BONITOBelum ada peringkat
- Nursing Management - Colon CancerDokumen7 halamanNursing Management - Colon CancerReese Alessandra GandulfoBelum ada peringkat
- English Nursing: Have You Gave A Chamber Pot To Mrs. Johnson?Dokumen2 halamanEnglish Nursing: Have You Gave A Chamber Pot To Mrs. Johnson?Faris Albert WenasBelum ada peringkat
- Medication To Manage Abortion and MiscarriageDokumen8 halamanMedication To Manage Abortion and MiscarriageNisaBelum ada peringkat
- Chest Wall, Lung, Mediastinum, and Pleura ProceduresDokumen124 halamanChest Wall, Lung, Mediastinum, and Pleura ProceduresKenn BrillanteBelum ada peringkat
- English Intervention DialogueDokumen3 halamanEnglish Intervention DialogueJihan Irbah TrianiBelum ada peringkat
- ICU Accomplishment Report and Improvement PlanDokumen5 halamanICU Accomplishment Report and Improvement PlanMikhaelEarlSantosTacordaBelum ada peringkat