Anda mungkin juga menyukai
- Nstemi (Non ST Elevation Myocardial Infarction)Dokumen37 halamanNstemi (Non ST Elevation Myocardial Infarction)andi yusmawatiBelum ada peringkat
- SEC A GP 1 OsamaDokumen16 halamanSEC A GP 1 OsamaAiman SiddiquiBelum ada peringkat
- Risk Stratification Flowchart - 1Dokumen4 halamanRisk Stratification Flowchart - 1wuddafrenBelum ada peringkat
- Lecture 12 Cardio Intensive CasesDokumen32 halamanLecture 12 Cardio Intensive Casesraul0% (1)
- Unit Task Cardiovascular ChangesDokumen3 halamanUnit Task Cardiovascular ChangesCamille MactalBelum ada peringkat
- Nursing Management of Acute Myocardial InfarctionDokumen43 halamanNursing Management of Acute Myocardial InfarctionRizka Patria SariBelum ada peringkat
- Cardiopulmonary: Hafsa Siddiqui Ifrah Laiq Maham Fazal Ur RahmanDokumen29 halamanCardiopulmonary: Hafsa Siddiqui Ifrah Laiq Maham Fazal Ur RahmanSalman KhanBelum ada peringkat
- Chapter 1.2 Algorithym of Risk StratificationDokumen26 halamanChapter 1.2 Algorithym of Risk StratificationMUHAMMAD DANISH AMIN BIN BORHANUDDINBelum ada peringkat
- PBL 2 Session 2 PresentationDokumen44 halamanPBL 2 Session 2 PresentationElisaBelum ada peringkat
- Case Study: Congestive Heart FailureDokumen7 halamanCase Study: Congestive Heart FailureXI-E / 21 / MARY TRIANABelum ada peringkat
- Cardiovascular System Review: Valve Disease, Syncope, Heart FailureDokumen1 halamanCardiovascular System Review: Valve Disease, Syncope, Heart FailurecocoBelum ada peringkat
- Drugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3Dokumen47 halamanDrugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3DR Muhammad Abdul BasitBelum ada peringkat
- Understanding Cardiovascular DisordersDokumen77 halamanUnderstanding Cardiovascular DisordersSaraBelum ada peringkat
- Dr. Reham LecturesDokumen35 halamanDr. Reham LecturesSoad RedaBelum ada peringkat
- Ischemic Stroke g6Dokumen8 halamanIschemic Stroke g6Kistnah Cassandra GapolBelum ada peringkat
- Arizmendi G72 T10Dokumen6 halamanArizmendi G72 T10IrvinSerranoJBelum ada peringkat
- Cardiac Rehab Goals BenefitsDokumen15 halamanCardiac Rehab Goals BenefitsammarmashalyBelum ada peringkat
- Heart Disease-The Silent Killer: by Dr. Muhammad AsifDokumen35 halamanHeart Disease-The Silent Killer: by Dr. Muhammad AsifMuhammad AsifBelum ada peringkat
- Nursing Care of Clients With Cardiovascular DisorderDokumen16 halamanNursing Care of Clients With Cardiovascular DisorderLuna MarieBelum ada peringkat
- Unstable Angina Pectoris High Risk + Post ASD Closure: Case PresentationDokumen27 halamanUnstable Angina Pectoris High Risk + Post ASD Closure: Case PresentationmohadriaBelum ada peringkat
- Nursing Study GuideDokumen21 halamanNursing Study GuideYanahBelum ada peringkat
- Case 3 Ms Rle ArcayanDokumen11 halamanCase 3 Ms Rle ArcayanVictoria Mae Irong CabahugBelum ada peringkat
- Coronary Artery Disease: Causes, Symptoms, and TreatmentDokumen7 halamanCoronary Artery Disease: Causes, Symptoms, and Treatmentcali kBelum ada peringkat
- Congestive Cardiac Failure GuideDokumen47 halamanCongestive Cardiac Failure GuideRajesh Sharma100% (1)
- Heart Failure: Scott Kaba MatafwaliDokumen25 halamanHeart Failure: Scott Kaba MatafwaliAngetile KasangaBelum ada peringkat
- Clinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzDokumen31 halamanClinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzNoreenBelum ada peringkat
- heart failure الاخيرDokumen30 halamanheart failure الاخيرAliBelum ada peringkat
- Case Study 3 - HCVDDokumen12 halamanCase Study 3 - HCVDJilkiah Mae Alfoja CampomanesBelum ada peringkat
- Ischemic Heart DiseaseDokumen56 halamanIschemic Heart DiseaseSMART PHARMACY By BRIJESHBelum ada peringkat
- ICM 5 Cases 1 - 12Dokumen76 halamanICM 5 Cases 1 - 12oyim sBelum ada peringkat
- PrintDokumen28 halamanPrintPaul TorrecampoBelum ada peringkat
- Congestive Heart FailureDokumen39 halamanCongestive Heart FailureEthiopia TekdemBelum ada peringkat
- Assessment & Reasoning Cardiac System: Suggested Cardiac Nursing Assessment Skills To Be DemonstratedDokumen8 halamanAssessment & Reasoning Cardiac System: Suggested Cardiac Nursing Assessment Skills To Be DemonstratedSharon Tanveer100% (1)
- HypertensionDokumen36 halamanHypertensionmohamedahmedf12345678Belum ada peringkat
- How to Screen for and Prevent Cardiopulmonary ConditionsDokumen38 halamanHow to Screen for and Prevent Cardiopulmonary ConditionsArham ShamsiBelum ada peringkat
- What Are The Signs and Symptoms of Heart Failure?Dokumen4 halamanWhat Are The Signs and Symptoms of Heart Failure?Lara TechiesBelum ada peringkat
- Hypotention مDokumen7 halamanHypotention مSophy YounanBelum ada peringkat
- Hypertensive Urgency: PGI Jorge John III P. QuilalaDokumen32 halamanHypertensive Urgency: PGI Jorge John III P. QuilalaJerome GeronimoBelum ada peringkat
- Cardiac Condition NCM 112Dokumen10 halamanCardiac Condition NCM 112Irish Eunice FelixBelum ada peringkat
- HNW CHP # 3Dokumen39 halamanHNW CHP # 3zaraali2405Belum ada peringkat
- Sabina Week 3 STEMI Case Study 4Dokumen11 halamanSabina Week 3 STEMI Case Study 4sapanjeet kourBelum ada peringkat
- Kuliah Pakar HF FKUMMDokumen46 halamanKuliah Pakar HF FKUMMOkta Dwi Kusuma AyuBelum ada peringkat
- Left-Sided Heart Failure - Symptoms, Causes and TreatmentDokumen14 halamanLeft-Sided Heart Failure - Symptoms, Causes and TreatmentHanzala Safdar AliBelum ada peringkat
- Approach To Cardiovascular Diseases in MCPS-MRCGP Part 1-MinDokumen109 halamanApproach To Cardiovascular Diseases in MCPS-MRCGP Part 1-Minbatew72175Belum ada peringkat
- CardiologyDokumen9 halamanCardiologyAbi RajasingamBelum ada peringkat
- Hypertension 101028172250 Phpapp01Dokumen17 halamanHypertension 101028172250 Phpapp01gil gomzBelum ada peringkat
- Welcome To AIIMSDokumen104 halamanWelcome To AIIMSKaramsi Gopinath NaikBelum ada peringkat
- Group 5 HFDokumen21 halamanGroup 5 HFJerson Aizpuro SuplementoBelum ada peringkat
- Atrial Fibrillation: Dr. Roaa AlamoudiDokumen15 halamanAtrial Fibrillation: Dr. Roaa AlamoudiRana AlmimoniBelum ada peringkat
- STEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimDokumen33 halamanSTEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimAnwar Mo SajaBelum ada peringkat
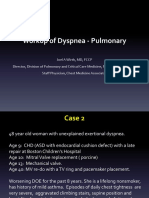
- DyspneaDokumen35 halamanDyspneaEnvhy AmaliaBelum ada peringkat
- Drugs in Sports: Effects, Health Implications and LegalityDokumen15 halamanDrugs in Sports: Effects, Health Implications and LegalityMalabaris Malaya Umar SiddiqBelum ada peringkat
- Geria - CardioDokumen4 halamanGeria - CardioLeah GordoncilloBelum ada peringkat
- Myocardial InfarctionDokumen10 halamanMyocardial InfarctionDaniel GeduquioBelum ada peringkat
- Cardio-Vascular Problems: Group 1Dokumen15 halamanCardio-Vascular Problems: Group 1Reanne Claudine LagunaBelum ada peringkat
- Heart Failure-MedscpeDokumen104 halamanHeart Failure-Medscpealicenyaga554Belum ada peringkat
- Creatin. Creatin. Creatin. Creatin. Creatin. CreatinDokumen2 halamanCreatin. Creatin. Creatin. Creatin. Creatin. CreatinEna PaparićBelum ada peringkat
- "Sports Medicine. Medical Control. The Methods of Sportsmen InvestigationDokumen24 halaman"Sports Medicine. Medical Control. The Methods of Sportsmen InvestigationLatika ChoudhuryBelum ada peringkat
- Coronary Artery Disease: By. Saiha AlinaDokumen19 halamanCoronary Artery Disease: By. Saiha AlinasaihaBelum ada peringkat
- The Amazing Way to Reverse Heart Disease Naturally: Beyond the Hypertension Hype: Why Drugs Are Not the AnswerDari EverandThe Amazing Way to Reverse Heart Disease Naturally: Beyond the Hypertension Hype: Why Drugs Are Not the AnswerPenilaian: 5 dari 5 bintang5/5 (2)
- Material Balance Laboratory: Ice Cream Process III. Equipment: IV. MaterialsDokumen5 halamanMaterial Balance Laboratory: Ice Cream Process III. Equipment: IV. MaterialsMaurice HadawayBelum ada peringkat
- Nutrition & Dietetics (Dietician) Careers - Courses, Jobs & SalaryDokumen10 halamanNutrition & Dietetics (Dietician) Careers - Courses, Jobs & SalaryPrakash ChavanBelum ada peringkat
- MANAGEMENT GUIDE FOR LAYER PARENT STOCKDokumen45 halamanMANAGEMENT GUIDE FOR LAYER PARENT STOCKLilisBelum ada peringkat
- DR Mariza - Top 10 Inflammatory Foods ReportDokumen11 halamanDR Mariza - Top 10 Inflammatory Foods ReportMitchellFelixBelum ada peringkat
- Pathophysiology of cholangiocarcinomaJAYCERDokumen3 halamanPathophysiology of cholangiocarcinomaJAYCERirish_estrellaBelum ada peringkat
- The Perfect Answer Revision Guide CIE IGCSE Biology 2Dokumen53 halamanThe Perfect Answer Revision Guide CIE IGCSE Biology 2Bob100% (4)
- Ote 9 10 11 18Dokumen14 halamanOte 9 10 11 18Thanh Thúy Vũ ThịBelum ada peringkat
- Oferit de Retete Culinare Romanesti.: Denumire Calorii Proteine Lipide GlucideDokumen36 halamanOferit de Retete Culinare Romanesti.: Denumire Calorii Proteine Lipide GlucideLudmila GraurBelum ada peringkat
- Proposal SampleDokumen8 halamanProposal SampleAndre KristantoBelum ada peringkat
- Progressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes MellitusDokumen7 halamanProgressive Muscle Relaxation (PMR) Is Effective To Lower Blood Glucose Levels of Patients With Type 2 Diabetes Mellituseno wijayaBelum ada peringkat
- 8 Week HIIT Fat Burning Workout ProgramDokumen1 halaman8 Week HIIT Fat Burning Workout ProgramOkanBelum ada peringkat
- Waist To Hip RatioDokumen7 halamanWaist To Hip RatioYiu Nam SoBelum ada peringkat
- FaddietassignmentdetailsrubricDokumen2 halamanFaddietassignmentdetailsrubricapi-357189210Belum ada peringkat
- 1 PemDokumen30 halaman1 PemFaisal Ibn MushtaqBelum ada peringkat
- Nutritional Treatments For Opioid AddictionDokumen4 halamanNutritional Treatments For Opioid AddictionEnzoBelum ada peringkat
- Gastric CancerDokumen57 halamanGastric CancerAinAlan Hafifi100% (1)
- SURGICAL NUTRITION GUIDEDokumen59 halamanSURGICAL NUTRITION GUIDEPrincewill SeiyefaBelum ada peringkat
- Identify Nutrients Gizmos-Air PodsDokumen4 halamanIdentify Nutrients Gizmos-Air Podsapi-398397642Belum ada peringkat
- Cause and Effect Connectives in Medical WritingDokumen3 halamanCause and Effect Connectives in Medical Writingraden bayuBelum ada peringkat
- Bacterial Flora in Digestive Disease Focus On Rifaximin C. Scarpignato Et. Al. Karger 2008 WWDokumen156 halamanBacterial Flora in Digestive Disease Focus On Rifaximin C. Scarpignato Et. Al. Karger 2008 WWFantasyoflove VallyBelum ada peringkat
- Feasibility Study - Restaurant Sample Business Plan OutlineDokumen18 halamanFeasibility Study - Restaurant Sample Business Plan OutlineNewman Enyioko50% (2)
- Mens Fitness UK - March 2016Dokumen180 halamanMens Fitness UK - March 2016Raphael Doukkali100% (3)
- Protocolo Da BombaDokumen52 halamanProtocolo Da BombaEmerson SaBelum ada peringkat
- Mojfpt 06 00176 PDFDokumen2 halamanMojfpt 06 00176 PDFSreevidyasreeBelum ada peringkat
- Body Shape QuestionnaireDokumen2 halamanBody Shape QuestionnaireCaleb Sylvester100% (2)
- Relationship Between Healthy Behavior and Health Status in Kelurahan UjungDokumen11 halamanRelationship Between Healthy Behavior and Health Status in Kelurahan UjungMoken JamcoBelum ada peringkat
- Native Potatoes From The Andes: New Health Foods and Gourmet DelightsDokumen2 halamanNative Potatoes From The Andes: New Health Foods and Gourmet DelightsHelton SilvaBelum ada peringkat
- Liver TransplantationDokumen6 halamanLiver TransplantationPriyaBelum ada peringkat
- Maternity Nursing ReviewDokumen8 halamanMaternity Nursing ReviewJulienne Sanchez-Salazar100% (2)
- A Case Study of Consumer Motivation in Organic Food Consumption From Costales Nature Farms in Majayjay, LagunaDokumen29 halamanA Case Study of Consumer Motivation in Organic Food Consumption From Costales Nature Farms in Majayjay, LagunaDanna DelalamonBelum ada peringkat