Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Quality of Operation Notes Audit PresentationDokumen31 halamanQuality of Operation Notes Audit PresentationPushpinder Singh SandhuBelum ada peringkat
- Long Term Scheduling For Optimal Sizing of Renewable Energy Sources For HospitalsDokumen9 halamanLong Term Scheduling For Optimal Sizing of Renewable Energy Sources For HospitalsMadusanka WeebeddaBelum ada peringkat
- Mindray BC 5380 Auto Hematology AnalyzerDokumen2 halamanMindray BC 5380 Auto Hematology AnalyzerMadusanka WeebeddaBelum ada peringkat
- Air Conditioner: Owner'S ManualDokumen40 halamanAir Conditioner: Owner'S ManualMadusanka WeebeddaBelum ada peringkat
- V5 Brochure May 2020Dokumen2 halamanV5 Brochure May 2020Madusanka WeebeddaBelum ada peringkat
- An Optimal Power Scheduling Method For Demand Response in Home Energy Management SystemDokumen10 halamanAn Optimal Power Scheduling Method For Demand Response in Home Energy Management SystemMadusanka WeebeddaBelum ada peringkat
- Bidding Document - SBD 03 CorrectedDokumen17 halamanBidding Document - SBD 03 CorrectedMadusanka WeebeddaBelum ada peringkat
- Product Data Sheet: PRD40 Modular Surge Arrester - 3 Poles + N - 340VDokumen2 halamanProduct Data Sheet: PRD40 Modular Surge Arrester - 3 Poles + N - 340VMadusanka WeebeddaBelum ada peringkat
- English EngineeringDokumen1 halamanEnglish EngineeringMadusanka WeebeddaBelum ada peringkat
- S Scchhooooll Ffoooodd D Diiaarryy: Example: Snack FoodDokumen5 halamanS Scchhooooll Ffoooodd D Diiaarryy: Example: Snack FoodMadusanka WeebeddaBelum ada peringkat
- Ceylon Electricity Board: Vacancies of Electrical / Civil Superintendents - NTDND & EI ProjectDokumen4 halamanCeylon Electricity Board: Vacancies of Electrical / Civil Superintendents - NTDND & EI ProjectMadusanka WeebeddaBelum ada peringkat
- National Registration and Grading Scheme For Construction ContractorsDokumen4 halamanNational Registration and Grading Scheme For Construction ContractorsMadusanka WeebeddaBelum ada peringkat
- Product Environmental Profile: Switch 63A 2P BiconnectDokumen5 halamanProduct Environmental Profile: Switch 63A 2P BiconnectMadusanka WeebeddaBelum ada peringkat
- CHPB - Prospectus 2021Dokumen35 halamanCHPB - Prospectus 2021Madusanka WeebeddaBelum ada peringkat
- Dedefr VFDRFDokumen8 halamanDedefr VFDRFMadusanka WeebeddaBelum ada peringkat
- Tamil-Engineering 2Dokumen1 halamanTamil-Engineering 2Madusanka WeebeddaBelum ada peringkat
- Telephone DirectoryDokumen44 halamanTelephone DirectoryMadusanka Weebedda100% (1)
- Req - 10546 - 003705 - 001 Oi-4408 MR Prabuddha PDFDokumen3 halamanReq - 10546 - 003705 - 001 Oi-4408 MR Prabuddha PDFMadusanka WeebeddaBelum ada peringkat
- Lighting Design by Lumen Method (With Examples) - LinkedinDokumen15 halamanLighting Design by Lumen Method (With Examples) - LinkedinMadusanka WeebeddaBelum ada peringkat
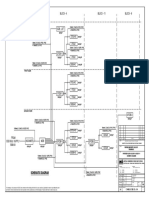
- Block - 4 Block - 11 Block - 6: Schematic DiagramDokumen1 halamanBlock - 4 Block - 11 Block - 6: Schematic DiagramMadusanka WeebeddaBelum ada peringkat
- Eg8 Geo Chapter04Dokumen17 halamanEg8 Geo Chapter04Madusanka WeebeddaBelum ada peringkat
- Upper Floor-Electric PDFDokumen2 halamanUpper Floor-Electric PDFMadusanka WeebeddaBelum ada peringkat
- Table 4D1A PDFDokumen1 halamanTable 4D1A PDFMadusanka Weebedda100% (1)
- Assignment 2 - MHZ5530 2017-18Dokumen2 halamanAssignment 2 - MHZ5530 2017-18Madusanka WeebeddaBelum ada peringkat
- Space-Vector PWM With TMS320C24x/F24x Using Hardware and Software Determined Switching PatternsDokumen44 halamanSpace-Vector PWM With TMS320C24x/F24x Using Hardware and Software Determined Switching PatternsMadusanka WeebeddaBelum ada peringkat
- Faculty of Engineering Technology: Office Use OnlyDokumen9 halamanFaculty of Engineering Technology: Office Use OnlyMadusanka WeebeddaBelum ada peringkat
- AdenomyosisDokumen1 halamanAdenomyosisVictor GomoiuBelum ada peringkat
- Ace ArsenalDokumen11 halamanAce ArsenalJustus WeißeBelum ada peringkat
- Bell's Palsy Treatments & Medications - SingleCareDokumen11 halamanBell's Palsy Treatments & Medications - SingleCareRoxan PacsayBelum ada peringkat
- Unani Product List PDFDokumen109 halamanUnani Product List PDFAK50% (2)
- Mommy's MedicineDokumen3 halamanMommy's Medicinekcs.crimsonfoxBelum ada peringkat
- HfiDokumen4 halamanHfiakalaw3Belum ada peringkat
- Leaflet - Augmentin - Tab - SuspDokumen17 halamanLeaflet - Augmentin - Tab - SuspagrocarlisacBelum ada peringkat
- The Restoration of Endodontically Treated, Single-Rooted Teeth With Cast or Direct Posts and Cores A Systematic ReviewDokumen7 halamanThe Restoration of Endodontically Treated, Single-Rooted Teeth With Cast or Direct Posts and Cores A Systematic ReviewLuis Alberto Carpio MorenoBelum ada peringkat
- Pathfinder 2nd Edition House Rules Compendium - GM BinderDokumen119 halamanPathfinder 2nd Edition House Rules Compendium - GM BinderBrandon PaulBelum ada peringkat
- En PIL BetmigaDokumen6 halamanEn PIL BetmigaEmma KateBelum ada peringkat
- Ownership, Operation, Maintenance, and Inspection of Amusement Rides and DevicesDokumen4 halamanOwnership, Operation, Maintenance, and Inspection of Amusement Rides and DevicesMarlon Piarpuito Enriquez0% (1)
- JMM 29 119Dokumen8 halamanJMM 29 119subanant11Belum ada peringkat
- Anatomy & Physiology Unit 1Dokumen29 halamanAnatomy & Physiology Unit 1Priyanjali SainiBelum ada peringkat
- Site-Specific and Stoichiometric Modification of Antibodies by Bacterial TransglutaminaseDokumen3 halamanSite-Specific and Stoichiometric Modification of Antibodies by Bacterial Transglutaminasespamemail00Belum ada peringkat
- CELECOXIBDokumen1 halamanCELECOXIBRicky Ramos Jr.Belum ada peringkat
- Procedure For Penicillin Skin TestingDokumen4 halamanProcedure For Penicillin Skin TestingHarshan Isuru KumaraBelum ada peringkat
- RetailerPriceList OHDokumen1 halamanRetailerPriceList OHMuhammad Samiur RahmanBelum ada peringkat
- Operative Hand InstrumentsDokumen22 halamanOperative Hand InstrumentsSharad Banker50% (2)
- Hap-1 Question Paper 2018-19 1st SemesterDokumen1 halamanHap-1 Question Paper 2018-19 1st SemesterLavanya Tanguturi yellaBelum ada peringkat
- USMLE - VirusesDokumen120 halamanUSMLE - Viruseszeal7777100% (1)
- Medical Decision MakingDokumen14 halamanMedical Decision MakingwbothaBelum ada peringkat
- Diuretics Antidiabetics AnalgesicsDokumen7 halamanDiuretics Antidiabetics AnalgesicsBillQueBelum ada peringkat
- ALP Crestline PDFDokumen2 halamanALP Crestline PDFJashmyn JagonapBelum ada peringkat
- ENT Summery TABLEDokumen19 halamanENT Summery TABLEtaliya. shvetzBelum ada peringkat
- Actalyke Mini Op Man D6500091JDokumen29 halamanActalyke Mini Op Man D6500091Jjyoti ranjanBelum ada peringkat
- Orthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceDokumen1 halamanOrthotic/Prosthetic Referral Form: Dispensing RX: Please Evaluate and Treat Patient With The Following DeviceKelly Roberts WiggenBelum ada peringkat
- Uniformity of Dosage UnitsDokumen5 halamanUniformity of Dosage UnitsJai MurugeshBelum ada peringkat
- Doh DC 2018-0142Dokumen2 halamanDoh DC 2018-0142vanceBelum ada peringkat